Open Access
Case Report
Max Screen >>
ISSN: 2455-7617
Copyright: © 2016 Pataki I. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
We would like to present two patients with triple localized, synchronous colon tumors who underwent emergency operations for obstruction. The second and third localizations were discovered during the operation.
Keywords: Triple synchronous tumors; Bowel obstruction
Using PubMed we found a diversity of publications referring to multiple colon tumors. Some of them defined synchronous tumors as affected large bowel sites alternating with healthy sections. The triple localization of colon tumors is a very rare condition.
In 2011, a 55 year old male patient was examined at the Internal Medicine Ward for diffuse abdominal cramps felt for already six months. He complained of fatigue, and moderate anemia was found. Other laboratory findings were irrelevant. A colonoscopy was performed and a stenotic tumor was found at 20 cm from the anal verge. The endoscope could not be passed through the tumorous site. Bowel obstruction symptoms developed a couple of hours after the examination.
We performed an emergency midline laparotomy. Beside the known stenotic tumor, we found another tumor expansively growing on the caecum. A right hemicolectomy and a segmental resection of the recto-sigmoid tumor were performed. During the mobilization of the descending colon we found the third tumor hiding in the splenic flexure. We removed it by another segmental colectomy. Bowel continuity was established by ileo-transversostomy and two end to end colo-colic anastomosis(Figure 1). The elongated sigmoid colon was very helpful in the reconstruction process. We finished the operation with a loop-ileostomy in order to avoid anastomotic leakage. The patient was discharged on the ninth postoperative day. His histological finding concluded pT3N1Mx, Dukes C, Astler-Coller C2 staging. As for genetics, mutation on the KRAS gene, exon 2 was described. Our patient underwent chemotherapy and after 8 months, and then he was readmitted to the surgical ward. His chest and abdominal CT’s, tumor markers and colonoscopy findings showed normal parameters, so we suspended the loop-ileostomy. He continued chemotherapy (altogether 12 sessions with FOLFOX) and had colonoscopy and CT every year. He has been tumor free for almost 4 years.
Another male patient was examined at the Internal Medicine Ward in 2014. The 62 year old man was known as an alcohol consuming, cirrhotic patient. Laboratory findings confirmed this status. A colonoscopy was performed in order to verify his mild abdominal complains. The tumors were localized at 5 cm and 50 cm from the anal verge. The latter one was stenosing. Also, a couple of hours later, symptoms of bowel obstruction developed, forcing us to perform an emergency midline laparotomy. A left hemicolectomy was done, closing the anal canal using Hartmann’s procedure. After removing the gases and feces from the proximal colon site, we found the third tumor near the hepatic flexure, which was also removed. The ascending large bowel served for colostomy. His histological finding corresponded to pT3N2Mx, Dukes C, Astler–Coller C2 stage. A mutation on KRAS gene exon 2 was also found. We discharged this patient on the 13th postoperative day. His follow-up was difficult due to social problems. He died one month later in a hospice. On autopsy, liver metastasis was confirmed, and the staging became pT3N2M1.
The occurrence of double localization of colon tumors is estimated at around 1-8% [1-4], but triple synchronous tumors are rarer conditions [5]. The second tumor site is discovered mainly during emergency laparotomy [2]. Precise diagnosis localizing synchronous tumor sites can be made only when bowel obstruction is imminent. (wait and see ) PET-CT colonography may be very helpful when total colonoscopy is not available or stenosing lesion is found [6]. As far as we know, these cases are the first ones published from Hungary.

![]()

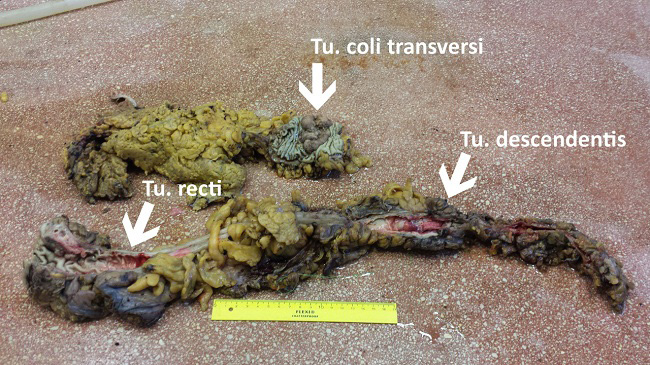 |
| Figure 1: The pathological findings of the second patient |




































