Open Access
Research Article
Max Screen >>
ISSN: 2455-7617
Copyright: © 2015 Jacob N. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Purpose: The posterior approach to the hip joint involves operating in close proximity to the sciatic nerve. Iatrogenic injury to the sciatic nerve has been reported to occur in 0.6 - 1.9% of cases [1]. Stretching, transection or suturing of the nerve may occur during access or while closing the capsule and short external rotators to the hip.
The position of the Sciatic nerve is variable, and this study aims to look for the correlation between femoral head size and the distance to the sciatic nerve in order to be able to judge position during the posterior approach to the hip.
Methods: 60 Magnetic Resonance Imaging Scans of Hips were identified to examine for position of the sciatic nerve in relation to insertion of obturator externus and the postero-medial corner of the lesser trochanter. The relationship with the femoral head size was also examined
Results: The results show that with increasing size of femoral head, the distance to the sciatic increases. The average distances to the Sciatic Nerve from the lesser trochanter was 14.9mm when head size was greater than 45mm and was 13.1mm when head size was below 45mm.
Conclusions: There is a proportional increase in distance of sciatic nerve from the hip joint with increase in femoral head size. This study provides evidence on relationship of the nerve to the hip joint which further strengthens our understanding of anatomy and we hope will help to give surgeons a good idea of the proximity of the nerve to their operative field.
Keywords: Sciatic Nerve; Posterior Approach; Hip Arthoplasty; Nerve injury
The sciatic nerve is at risk especially during posterior approach to the hip joint because of close proximity during dissection.
The sciatic nerve is the longest and widest single nerve in the body. It arises from the lumbo-sacral plexus. It arises from spinal nerves from L4 through to S3. It consists of common peroneal and tibial divisions [2,3].
The nerve exits the pelvis through the greater sciatic foramen, running deep to the piriformis muscle. It runs down the thigh between the greater trochanter and the ischial tuberosity, and commonly divides into its main terminal branches – The common peroneal and the tibial nerves, at the level of the mid-thigh.
With the patient in the lateral decubitus position, starting the skin incision posterior to the lateral side of the greater trochanter, carry it distally about 6 cm along the femoral axis. Proximally, the incision runs slightly curved towards the Posterior Superior Iliac Spine to a point approximately 6 cm proximal to the greater trochanter. The fascia lata and gluteal muscle is then incised in-line with the skin incision.
Retraction of the gluteal muscle flap posteriorly reveals the short external rotators of the hip. The sciatic nerve can be palpated posteriorly in the wound. Its exposure is not necessary for uncomplicated hip arthroplasty, but the surgeon should be aware of the location.
Stay sutures are placed for retraction and subsequent repair in the tendons of the short external rotators. Reflection of the short rotator muscles exposes the hip capsule [4,5].
Both retraction of the gluteal muscle flap and placement of stay sutures in the short external rotator tendons are points during surgery when the sciatic nerve are most at risk.
The studies assessing the position of the sciatic nerve in relation to the hip joint are quite limited, but identification may have multiple clinical benefits including avoiding iatrogenic nerve injury and for localisation for peripheral nerve blocks.
Magnetic resonance Imaging (MRI) scans of hip joints performed in 2010 were identified using the PACS image viewer system at a district general hospital and included in this study.
MRI scans were excluded if a) The scan did not include below the level of the lesser trochanter b) Anatomy may have been
distorted by surgery such as hip replacement surgery c) Patients under 18 years old.
A single reviewer simultaneously examined the scans in both coronal and axial planes to identify the following:
1. Insertion of obturator externus (OE) (Figure 1a)
2. Postero-medial corner of the lesser trochanter (LT) (Figure 2a)
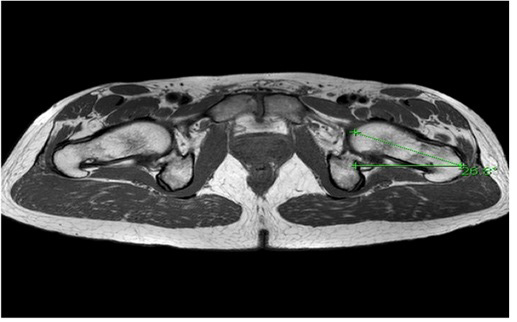
3. Position of the Sciatic Nerve (SN) (Figure 1b and 2b)
4. Femoral head size and (Figure 3)
5. Femoral neck anteversion (Figure 4)
All the above were identified and measurements made using the measurement tools provided on the image viewing software to obtain the relationship of the sciatic nerve in relation to these anatomical sites and correlation with femoral head size and neck anteversion.
The statistical analysis was performed using the student's t-test.
A total of 60 MRI scans performed over a one year period were included in the study. There were 16 males and 44 females, 30 were left hips and 30 were right hips. The average age of patient was 55 years. The average femoral head size was 45mm with an average anteversion of 14.4 degrees.
The average distance of the sciatic nerve to the postero-medial corner of the LT and the insertion of the OE insertion were 13.9mm and 34.6mm respectively. The average angles from the horizontal were 97.3 and 36.5 degrees from the LT and OE respectively. In 6 patients the sciatic nerve divided into branches above the level of the lesser trochanter. In these cases the measurements were taken from the closest branch.
The average distance to the sciatic nerve from the postero-medial corner of the LT when the femoral head size was less than 45mm was 13.1mm and when larger than 45mm was 14.9mm (p=0.3).
The average distance to the sciatic nerve from the OE insertion when femoral head size was less than 45mm was 31.5mm and when larger than 45mm was 38.7mm (p=0.0003).
The average distance of the sciatic nerve from the LT when femoral neck anteversion <14.4° was 12.4mm, and when neck anteversion >14.4° it was 15.3mm (p= 0.09).
The average distance of the sciatic nerve from the insertion of OE when femoral neck anteversion <14.4° was 35.8mm, and when neck anteversion >14.4° it was 33.5mm (p=0.3).
Although it is well documented that a posterior approach to the hip is associated with an increased risk of post-operative dislocation and iatrogenic nerve injury, it continues to be a popular choice as direct lateral and antero-lateral approaches are associated with upto 10% incidence of abductor weakness as well as heterotopic bone formation and femoral and obturator nerve injuries [6-8].
It therefore is important to have a good understanding of the location of the sciatic nerve in relation to the hip joint and its various anatomical landmarks during surgical dissection to the hip joint.
The results of the study show a statistically significant relationship between the femoral head size and the distance between the sciatic nerve and the OE insertion.
However, in general, this study provides the quite obvious conclusion that the smaller the femoral head size, the closer the sciatic nerve, and hence the higher the risk of injury to the nerve in the smaller patient.
A limitation of this study is that it does not take into account the position of the hip at the time of imaging. This is normally supine during imaging, whereas during surgery the patient is lateral, which is likely to affect the distance. However, the study still provides valuable information on the relative close proximity of the nerve.
Hip position has been previously found to affect the position of the nerve. Birke et al studied the effect of hip position in relation to ischial osteotomy during a pelvic triple or periacetabular osteotomy in the paediatric population. In the study involving MRI imaging they suggest the sciatic nerve moves away from the ischial osteotomy site on flexion of the hip to 30 to 45°, abduction and external rotation [9]. Dikici et al found that the sciatic nerve was in closest proximity to the middle part of the posterior acetabular rim in comparison with its superior and inferior parts, and this was more pronounced when the hip was flexed as compared to extended or neutral [10].
Superficial landmarks such as inguinal crease and femoral artery have been studied as markers to identify position of the sciatic nerve and ultrasound used to identify and depth and position measured at time of administration of nerve blocks. These studies have shown a fairly constant position of the nerve in relation to these landmarks (2.5 cm distal to the inguinal crease and 2.5 cm medial to the femoral artery and was directed posteriorly and laterally with a 10-15 degrees angle relative to the vertical plane) This position was unaffected by external rotation of the hip as compared to neutral [11].
In conclusion, we feel that in order to minimise complications related to a posterior approach to the hip joint, good clinical decision making on position of the nerve is absolutely vital. The size of the femoral head is easily acquired in clinic, based on X ray or CT and so it can be useful to judge the position of sciatic nerve for surgeons. However, the size of femoral head is not an independent factor and it should be analyzed along with other factors. This study provides evidence on relationship of the nerve to the hip joint which further strengthens our understanding of anatomy and we hope will help to give surgeons a good idea of the proximity of the nerve to their operative field and may also help in localising the nerve for the purpose of administering sciatic nerve blocks.

![]()

 |
| Figure 1a: View of right hip to identify insertion of OE |
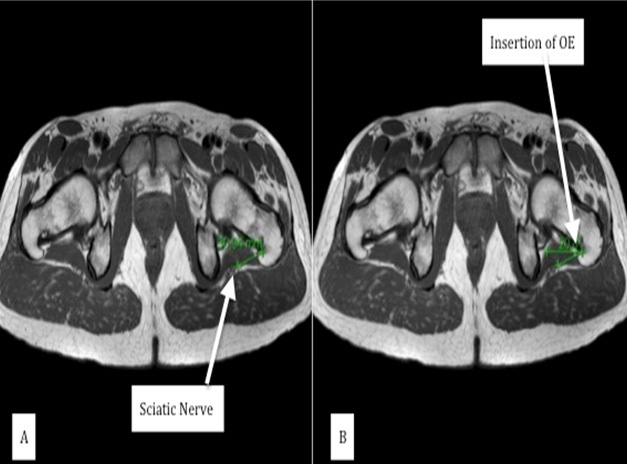 |
| Figure 1b: CloserView of right hip to identify the relationship between the OE and SN. Figure A shows the measurement of the distance from OE insertion to the sciatic nerve. Figure B shows the measurement of the angle from the horizontal of OE to the SN |
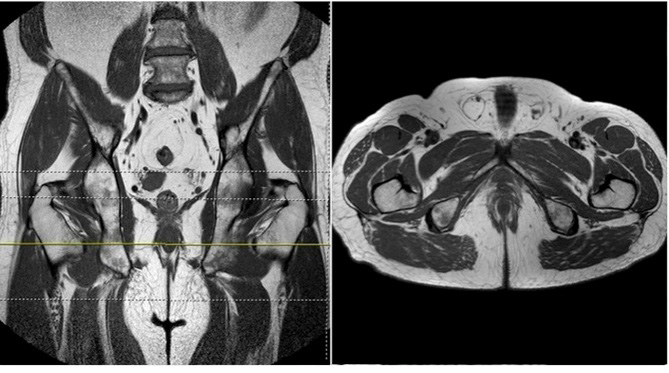 |
| Figure 2a: View of right hip to identify postero-medial corner of LT |
 |
| Figure 2b: View of axial slices of MRI of hips. Figure A shows the measurement of distance from LT to SN. Figure B shows how we identified the angle from horizontal of LT to SN |
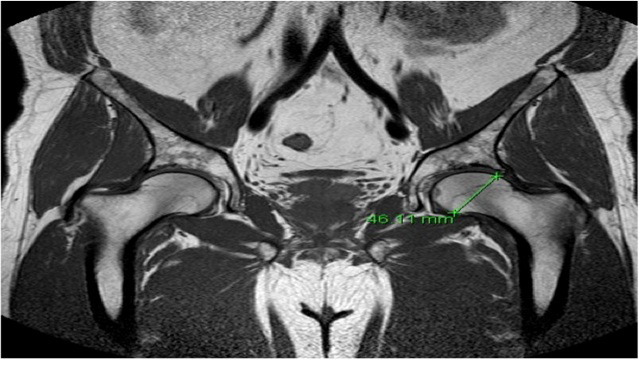 |
| Figure 3: View of coronal MRI of hips. The widest point of femoral head (head size) was measured using this view as demonstrated in the image |
 |
| Figure 4: View of sagittal MRI to identify anteversion. The image shows the anteversion of femoral neck with respect to a drawn neutral line which in this case measures 26.8 degrees |




































