Open Access
Research Article
Max Screen >>
ISSN: 2455-7633
Copyright: © 2016 Rafiee M. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background: Several studies have suggested that Insertion/Deletion polymorphism of ApoB gene is associated with obesity, dyslipidemia, diabetes and coronary heart disease (CHD). However, data are limited and inconsistence. The objective of this study is to investigate the aassociation between insertion/Deletion polymorphism of ApoB gene and dyslipidemia and obesity risk in patients with type 2 diabetes (T2D).
Method: In this cross-sectional study, 700 patients who suffer from T2D were recruited from referral centers of diabetes in Tehran. Height, weight and waist circumference were measured, and body mass index (BMI) was calculated. BMI greater than or equal to 30 is general obesity for both sexes. Also dyslipidemia is elevation of plasma total cholesterol (TC ≥ 200 mg/dl), or triglycerides (TG ≥ 150 mg/dl), or low-density lipoprotein (LDL-C ≥ 160 mg/dl), or a low high-density lipoprotein level (HDL < 50 in women and < 40 in men). Dietary intake was assessed by using a semi-quantitative food frequency questionnaire. The serum total cholesterol, triglycerides, HDL-c and LDL-c were determined enzymatically. ApoB genotyping was performed by 8% polyacrylamide gel electrophoresis.
Results: We have found that LDL-c level and LDL-c/HDL-c were significantly higher in men carriers Del allele than Ins/Ins, whereas that women carriers Del allele had higher TG level than Ins/Ins. Compare to Ins/Ins, carriers of the Del allele have general obesity risk and also hyper-LDL cholesterolemia and hypo-HDL cholesterolemia (OR = 1.65, P = 0.03; OR = 2.11, P = 0.01; OR = 2.72, P = 0.01, respectively).
Conclusion: The Del allele of ApoB gene could be a risk factor for general obesity and dyslipidemia in subjects with T2D.
Keywords: Apolipoprotien B; Ins/Del polymorphism; Dyslipidemia; Obesity; Diabetes
List of Abbrevations: ApoB: Apolipoprotein B; PCR: Polymerase chain reaction; FFQ: Food frequency questionnaire; HDL-c: High density lipoprotein cholesterol; LDL-c: Low density lipoprotein cholesterol; TG: Triglyceride; TC: Total cholesterol; CHD: Coronary heart disease; BMI: Body mass index; WC: Waist circumference; BF: Body fat; ANOVA: Analysis of variance; OR: Odd ratio; ANCOVA: Analysis of covariance
Type 2 diabetes (T2D) is a multifactorial disease that interacted with genetic and environmental factors [1]. Nearly 80% of those who have diabetes are obese and or have lipid profile abnormality [2]. However, the serum lipid levels and obesity are modulated by lifestyle. On the other hand genetic factors account for approximately 50% and 70% of the variance in dyslipidemia and obesity, respectively [3,4]. Disorders of lipid and lipoprotein are common complication of diabetic patients that increase the risk of coronary heart disease (CHD) [5]. Investigation of genome wide association studies reveals that some of genes involved in obesity and dyslipidemia [6]. ApoB gene is one of the most important genes that located on chromosome 2P, and contains 29 exons. ApoB is a main protein component of chylomicrons, VLDL and LDL lipoproteins, and acts as a ligand for LDL receptor to facilitate the uptake of serum cholesterol [7]. Hence, ApoB has a central role in lipid metabolism. Thus dyslipidemia is as a result in dysfunction of ApoB gene [8]. In the gene region of ApoB, several typical sites of single nucleotide polymorphisms have been observed that Insertion/Deletion (Ins/Del) is one of them. The Insertion/Deletion polymorphism is within the first exon. The frequent allele (93bp) encodes a 27 amino acid peptide (Ins; SP-27) and the deletion of 9bp results in 24 amino acid peptide (Del; SP-24) [9]. Investigations have shown that the correlation among Ins/Del polymorphism and lipid and lipoprotein levels may contribute to the pathogenesis of obesity, cardiovascular and non-alcoholic fatty liver disease [10,11]. Researchers demonstrated that the Del allele is associated with decrease secretion and increase degradation of ApoB [12]. Study of Benhizia et al. on rat hepatoma cells was showed that Ins allele carriers compare with Del/Del genotype have higher serum TG and VLDL levels [13]. However, several previous studies have reported that Del allele of ApoB gene associated with dyslipidemia, especially hyper-LDL- cholesterolemia [14,15]. Additionally, Saha, et al. has studied the association among the ApoB Ins/Del polymorphism and body mass index (BMI) in Hindi healthy population in Singapore and found that Del allele carriers have higher BMI compare with Ins/Ins homozygotes [16]. Previous studies have shown that different variants of Ins/Del polymorphism of ApoB gene are important genetic factors in obesity, mainly visceral obesity in non-diabetic subjects [11]. There is controversy between the results of a few studies in the world about the association of ApoB Ins/Del polymorphisms with obesity and dyslipidemia. This study was performed with notice to the fact that there is little and inconsistent information about probably role of different genetic variant ApoB Ins/Del polymorphism on development risk for dyslipidemia and obesity in patients with T2D.
As described in our previous study 700 patients with T2D (424 female and 276 male, 35-65 years) were studied [17]. All patients were randomly selected from the Iranian Diabetes Society and Gabric Diabetes Society or Health Centers, all located in Tehran. Diagnosis of diabetic patients was based on criteria including fasting blood glucose ≥ 126 mg/dl or consumption of drugs for diabetes treatment or both of them [18]. The study protocol was approved by the ethics committee of Tehran University of Medical Sciences and informed consent was obtained from each participant. Exclusion criteria included: (a) pregnancy, (b) lactation, (c) insulin injection.
Weight was measured without shoes and minimal clothing using a digital scale (Seca, Hamburg, Germany) with accuracy of 100 g. Height was measured without shoes using a stadiometer (Seca, Hamburg, Germany) with an accuracy of 0.5 cm. The waist circumference was measured by using non-elastic tape with an accuracy of 0.5 cm in the middle of the distance between last rib and iliac crest bone [19]. BMI was calculated as weight in kilograms divided by the square of height in meters. The WHO classifications were used for defining general obesity: BMI ≥ 30 kg/m2; and central obesity: WC ≥ 90 cm for men and ≥ 80 cm for women [20]. Body fat percentage was calculated by using Deurenberg formula and high body fat percentage is classified: BF% ≥ 25 for men and ≥ 33 for women [21]. Physical activity was also measured in terms of hours per day using the MET (metabolic-equivalent task) questionnaire which was developed and validated in previous studies in Europe [22]. In Iran, reliability and validity of the questionnaire have been confirmed by the Kelishadi, et al. study in adolescents Iran [23].
Dietary intake was estimated with the semi-quantitative food frequency questionnaire that was designed in Tehran Lipid and Glucose Study. This questionnaire includes 148 food items. Reliability and validity of the questionnaire have been confirmed [24]. Subjects are asked how often they consume each item per day, week, or month. Food-item intake frequencies are linked to nutrient data to estimate daily nutrient intakes. Nutritionist 3 (N3) software was used to calculate the amount of nutrient and total energy intake. Three categories of smoking status were used: current (including irregular smoking), former and never in last 6 month. Alcohol habits were divided into two categories including Individuals no and yes alcohol consumption during the last 6 month in the questionnaire.
Venous blood samples were collected after 12 hours fasting (overnight) in order to measure serum lipids and lipoprotein. Plasma total cholesterol (TC) and triglyceride (TG) concentration were measured using standard enzyme methods (Parsazmon, Karaj, Iran). Serum HDL-C and LDL-C were determined by turbidimetry automated on a Hitachiq21 analyzer (Roche, Hamburg, Germany). Dyslipidemia was characterized when TG ≥ 150 mg/dl, or TC ≥ 200 mg/dl, or LDL-C ≥ 160 mg/dl , or HDL-C < 40 mg/dl in men and < 50 mg/dl in women [25].
Genomic DNA was extracted by using salting out, as described previously [26]. PCR was performed in 25 μL mixture, containing 50 ng of gDNA, 0.2 mM of each primer (Forward: 5’-CAGCTGGCGATGGACCCGCCGA-3’; Reverse: 5’-ACCGGCCCTGGCGCCCGCCAGCA-3’), 2X Taq polymerase mix (SinaClon Bioscience Co.), and 7% Dimethyl sulfoxide (Sigma-Aldrich Co.) in 35 cycles of 94 oC for 50s and 64 oC for 90s. The PCR products were analyzed by 8% polyacrylamide gel electrophoresis, and subsequent staining by fluorescent red dyes (Biotium Inc.) [27].
SPSS version 18 was used for all statistical analysis (IBM SPSS Inc., Chicago, IL, USA). Data normality examined by Kolmogorove-Smirnove (K-S). Data were expressed as mean ± SD. Variables that have not normal distribution expressed to log-transformed. Independent sample t-test was used for comparing the means. Also, Analysis of Covariance (ANCOVA) was used to compare means after adjustment for confounding variables such as age, physical activity, family history of diabetes, alcohol consumption, smoking, Triglyceride, Total Cholesterol, BMI, antilipid medication, fiber intake and energy intake. We used logistic regression analysis to determine the association between ApoB Ins/Del variants and obesity risk after adjustment for confounding variables including age, physical activity, diabetes family history, smoking and energy intake, TG and TC, and also dyslipidemia risk after adjustment for age, physical activity, family history of diabetes, alcohol consumption, smoking, BMI, antilipid medication, fiber intake and energy intake. Odds ratios (ORs) and 95% confidence intervals (CIs( were calculated. Statistical analysis was performed separately for male and female. Recessive, dominant and co-dominant models were tested. Hardy-Weinberg equilibrium (HWE) was analyzed using X2 test. Also the significant level of P ≤ 0.05 was considered.
Table 1 displays the demographic, anthropometric and biochemical of participants. Figure 1 shows the PCR products of ApoB Ins/Del polymorphism on polyacrylamide gel electrophoresis. Genotypic frequency was: Ins/Ins: 67.1, Ins/Del: 29.5 and Del/Del: 3.4, that has been described [17].The genotype frequencies were in agreement with those predicted by the Hardy-Weinberg equilibrium (X2=0.046; p=0.977). The effects of dominant model were observed in both men and women of our study (Ins/Ins vs. Ins/Del + Del/Del). Multicollinearity analysis of all confounding variables suggests that there were no correlations between the variables (VIF=1). Table 2 shows the comparison of lipid levels and anthropometric measurements based on Ins/Del polymorphism of ApoB in women, men, and total population. Results showed that serum LDL-C concentration and LDL/HDL were significantly higher in men carrying the minor allele (Del) than in those with the Ins/Ins genotype (p=0.02 and p=0.04, respectively). In addition, Del allele carriers had higher means serum TG and LDL-c levels than homozygotes Ins/Ins in women and total population, respectively (p = 0.03 and p = 0.02, respectively). After adjustment for potential confounders including age, physical activity, family history of diabetes, alcohol consumption, BMI, smoking, antilipid medication intake, fiber and energy intake, the all above association remained significant (p < 0.05). No significant difference was observed between anthropometric measurement and ApoB Ins/Del polymorphism (p > 0.05). Table 3 shows the OR estimations of dyslipidemia and obesity for the ApoB Ins/Del polymorphism (dominant model) in men and women. We observed a statistically significant association between the ApoB Ins/Del polymorphism and hyper-LDL and hypo-HDL cholesterolemia in men and general obesity in women. Thus, men carriers of Del carriers had an approximately 1.98 and 2.45-fold risk of hyper-LDL and hypo-HDL Cholesterolemia compared with the Ins/Ins homozygotes, respectively (OR1 = 2.11; 95% CI: 1.18-3.76; p = 0.01, OR2 = 2.72; 95% CI: 1.22-6.05; p = 0.01, respectively. Furthermore, we observed that women carriers of Del allele had 1.65 fold higher general obesity risk, after adjustment for age, physical activity, family history of diabetes, alcohol consumption, smoking, energy intake, TG and TC compared with the Ins/Ins homozygotes (OR = 1.65; 95% CI 1.3-2.76, P = 0.03).
The importance of ApoB in lipid and lipoprotein metabolism is well established. Based on our knowledge, the present study was the first investigation to characterize associations between Ins/Del polymorphism of ApoB gene with obesity and dyslipidemia risk in diabetic population. We found no significant association between the ApoB Ins/Del polymorphism and anthropometric measurements. Furthermore, the present study shows that the polymorphism Ins/Del of ApoB gene is associated with higher serum levels of LDL-C and LDL/HDL in diabetic men and serum TG in diabetic women. These associations remained significant after adjusting for age, physical activity, family history of diabetes, alcohol consumption, BMI, smoking, antilipid medication intake, fiber and energy intake. The logistic regression analysis revealed that carriers of Del allele have significantly higher hyper-LDL cholestrolemia and hypo-HDL cholesterolemia risk only in men and general obesity risk only in women after adjustment for confounder variables. In agreement with our results, Saha, et al. reported that Del allele carriers of the Hindi healthy population are more obese than Ins/Ins genotype [16]. Also, Chun-fang, et al. showed that Del allele is associated with higher serum levels of TG, VLDL and obesity [28]. However, Benhizia, et al. in contrast to the results of our study exhibited that Ins allele is associated with higher risk of obesity [13]. Similar to our investigation, Lamia, et al. showed that carriers of Del allele had higher LDL-c concentration than subjects with Ins genotype [14]. Similarly, Halsall, et al. investigation on 725 non-diabetic British subjects indicated that TC and LDL-c levels were significantly higher in Del/Del homozygotes compare with carriers of Ins allele in men but not in women [15]. Also, Kammerer, et al. among the Mexican American families has been found that homozygotes for the Del allele had significantly higher mean levels LDL-C than Ins homozygotes [29]. The results from our study disagree with Tsunoda and Cavalli, et al. that exhibited no significant difference between ApoB Ins/Del polymorphism and lipid profile [30,31]. The findings of the present study indicate potential effects of the gene on dyslipidemia and obesity in patients with T2D. ApoB gene plays an important role in the metabolism of lipid and lipoproteIns by regulation of genes expression and transcription related with lipid [32,33]. Loss of 3 amino acids (leucine-alanine-leucine) in Del allele results in decrease hydrophobicity and displacement of the synthesized ApoB from endoplasmic network to cytoplasm, which has been observed to be related with dyslipidemia and obesity but mechanism is not well clear [34]. However, several experimental studies revealed that allele Del of ApoB gene through lower affinity and productions for LDL-receptor and VLDL, respectively result in reduced LDL clearance and increased TG in the liver [35]. Accordingly, accumulation of TG in carriers of Del allele in liver may result to uptake greater amount of TG by body tissues, especially adipose [36]. Researchers have demonstrated that liver TG and serum LDL-c concentration have a positive relation with the size and number of adipocytes [37]. This probabilistic mechanisms can cause for dyslipidemia and obesity risk in carriers of Del allele than homozygotes Ins/Ins. In fact, there is no clear mechanism that explains the association between ApoB Ins/Del polymorphism with anthropometric and blood lipid parameters. However, it can be attributed to the differences in the amount and type of sex hormones and fat distribution [38]. Some previous studies indicated that serum TG level is positively associated with general obesity only in women [39,40]. Accordingly it can be concluded that in women carriers of Del allele high TG level may result in development of general obesity. So association of this polymorphism with dyslipidemia and obesity is largely dependent to gender. This inconsistent results of studies in related with dyslipidemia and obesity risk and ApoB Ins/Del polymorphism may be because of gene-environmental interaction and different ethnicity. Some studies were focused on healthy population and or patients with cardiovascular diseases (CVD) [1,7-9]. Moreover, interaction of genes in different populations may cause different effects. Cross-sectional design of our study was main limitation that cannot express causality of this observed association. Additionally, the results of our study are associated with populations with T2D in Tehran, and cannot be generalized to the whole country and world. The existence of confounding variables in our studies may makes it difficult to estimate of the true association between ApoB Ins/Del polymorphism with the risk of dyslipidemia and obesity in patients with type 2 diabetes (T2D). In this study, factors such as age, physical activity, family history of diabetes, alcohol consumption, smoking, Ttriglyceride, Total Cholesterol, BMI, antilipid medication, fiber intake and energy intake often have an impact on dyslipidemia and obesity and so should be controlled. So, the major strength of our study was the determination of the actual association between dyslipidemia and obesity risk and Ins/Del polymorphism of ApoB gene after adjusted for confounding factors, which in previous studies were not considered. Further studies are suggested comparative studies as case- control to assess the impacts of different genotypes in healthy and non-healthy population. However the impact of ApoB Ins/Del polymorphisms has never been investigated in an Iranian population. So in this study, we assessed the association between ApoB Ins/Del polymorphisms and risk dyslipidemia and obesity in patients with T2D.
To sum up, data analysis showed that Del allele of ApoB gene can be considered as a risk factor for general obesity and high serum TG level in women and hyper-LDL cholesterolemia and hypo-HDL cholesterolemia in men with T2D. Therefore, lifestyle modification and weight and blood lipid parameters control are recommended for all people, especially for the individual carriers of Del allele.
This work was funded and supported by the Tehran University of Medical Sciences (Research project number 91-03-161-19322). The authors wish to thank the people who participated in this study.

![]()
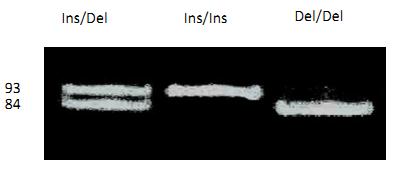 |
| Figure 1: Photograph of gel showing electrophoresis of fragment obtained after digestion of PCR-amplified, three genotype of the Apo-B Insertion/Deletion polymorphism are shown: Ins/Del, Ins/Ins and Del/Del |
Men (n=276) |
Women (n=424) |
All Subjects (n=700) |
||
Mean (SD) |
Mean (SD) |
p* |
Mean (SD) |
|
Age, year |
54.1 ± 6.6 |
53.8 ± 6.5 |
0.5 |
54 ± 6.5 |
Weight, kg |
81.7 ± 13.5 |
73.2 ± 13.4 |
<0.001 |
76.5 ± 14 |
Height, cm |
168.1 ± 8.6 |
156.7 ± 6.3 |
<0.001 |
161.3 ± 9.1 |
BMI, kg/m2 |
28.9 ± 4.1 |
29.7 ± 4.9 |
0.01 |
29.4 ± 4.6 |
WC, cm |
95.3 ± 9.9 |
90.5 ± 10.6 |
<0.001 |
92.3 ± 10.7 |
BF, % |
31.9 ± 5.1 |
42.7 ± 5.9 |
<0.001 |
37.2 ± 5.4 |
Physical activity, MET |
37.8 ± 6.3 |
37.7 ± 4.8 |
0.7 |
37.7 ± 5.4 |
Family history of diabetes, Yes% |
82 |
81 |
0.4 |
81.5 |
Alcohol consumption, Yes% |
6.5 |
1 |
<0.001 |
3 |
Smoking, Yes% |
20 |
15 |
0.02 |
17 |
Total energy intake, Kcal/day |
2818 ± 1119 |
2454 ± 828 |
0.4 |
2600 ± 970 |
TG, (x̄ ± SD (mg/dl), CV %)) |
152.9 ± 70.5, 46.1 |
156.3 ± 69.8, 44.6 |
0.5 |
155.0 ± 70.0, 45.1 |
TC, (x̄ ± SD (mg/dl), CV %)) |
185.2 ± 51.6, 27.8 |
196.8 ± 64.7, 32.8 |
0.01 |
192.1 ± 60.1, 31.2 |
LDL-C, (x̄ ± SD (mg/dl), CV (%)) |
108.2 ± 32.5, 30.03 |
109.8 ± 36.4, 35.1 |
0.5 |
109.1 ± 35.0, 32.08 |
HDL-C, (x̄ ± SD (mg/dl), CV (%)) |
49.8 ± 11.6, 23.29 |
55.0 ± 11.2, 20.3 |
<0.001 |
53.0 ± 11.7, 22.07 |
*Statistically significant differences between men and women ( independent sample t-test) |
||||
Men |
Women |
All Subjects |
||||||||||
Ins/Ins (n=191) |
Ins/Del+Del/Del (n=85) |
Ins/Ins (n=278) |
Ins/Del+Del/Del (n=146) |
Ins/Ins (n=469) |
Ins/Del+Del/Del (n=231) |
|||||||
Mean (SD) |
Mean (SD) |
p* |
p†,†† |
Mean (SD) |
Mean (SD) |
p* |
p†,†† |
Mean (SD) |
Mean (SD) |
p* |
p†,†† |
|
Weight,kg*,† |
81.7±13.8 |
81.6±12.9 |
0.8 |
0.7 |
73.8 ± 13.8 |
72 ± 12.6 |
0.1 |
0.1 |
77 ± 14.3 |
75.5 ± 13.5 |
0.1 |
0.3 |
Height, cm*,† |
168 ±8.4 |
167.5±9.1 |
0.4 |
0.3 |
156 ±6.19 |
156.7 ± 6.5 |
0.4 |
0.4 |
161.5 ±9.1 |
160.7 ± 9.2 |
0.2 |
0.5 |
BMI,Kgm2*,† |
28.8±4.2 |
29.06±3.95 |
0.6 |
0.2 |
29.3 ± 5.1 |
29.9 ± 4.5 |
0.1 |
0.08 |
29.5 ± 4.8 |
29.2 ± 4.3 |
0.4 |
0. 1 |
WC, cm*,† |
95.3±10.6 |
95.06±9.82 |
0.7 |
0.4 |
91 ± 11.1 |
89.5 ± 9.8 |
0.1 |
0.3 |
92.7 ± 10.9 |
91.6 ± 10.1 |
0.2 |
0.3 |
TG, mg/dl*, †† |
152.4 ± 74 |
153.9 ± 61.2 |
0.5 |
0.2 |
154.2 ± 70 |
166.8 ± 69 |
0.03 |
0.001 |
153 ± 71.8 |
158.2 ± 71.8 |
0.5 |
0.3 |
TC, mg/dl*,†† |
186.4 ± 48 |
182.6 ± 58.9 |
0.1 |
0.1 |
200 ± 58.2 |
205 ± 75 |
0.3 |
0.6 |
189.9 ± 54 |
196.7 ± 70.1 |
0.1 |
0.2 |
LDL-C, mg/dl*,†† |
104 ± 31.6 |
117.3 ± 33 |
0.02 |
0.001 |
109.9 ± 36 |
109.7 ± 37.4 |
0.7 |
0.8 |
107.4 ± 34 |
112.5 ± 35.9 |
0.02 |
0.01 |
HDL-C, mg/dl*,†† |
49 ± 11.5 |
51.6 ± 11.8 |
0.2 |
0.1 |
55.2 ± 11.1 |
54.7 ± 11.6 |
0.2 |
0.5 |
52.7 ± 11.6 |
53.5 ± 11.8 |
0.5 |
0.3 |
LDLC/HDL-C*,†† |
2.16 ± .57 |
2.4 ± .69 |
0.04 |
0.02 |
2 ± .69 |
2 ± .64 |
0.6 |
0.4 |
2 ± .64 |
2.1 ± .67 |
0.47 |
0.3 |
| - BMI, body mass index; WC, waist circumference; BF, body fat; TG: triglyceride; TC: total cholesterol; LDL-C: low density lipoprotein cholesterol; HDL-C: high density lipoprotein cholesterol *Independent sample t-test, unadjusted †P value determined by analysis of covariance (ANCOVA) after adjusted for age, physical activity, family history of diabetes, alcohol consumption, smoking, energy intake, Triglyceride and Total Colesterol ††P value determined by analysis of covariance (ANCOVA) after adjusted for age, physical activity, family history of diabetes, alcohol consumption, BMI, smoking, antilipid medication, fiber intake and energy intake Table 2: Comparison of anthropometric measurement and lipid profile between the two groups of Apo-B Ins/Del polymorphism in diabetic men and women |
||||||||||||
Dominant model: Ins/Ins vs. Ins/Del + Del/Del |
Men |
Women |
All subjects |
|||
OR (95% CI) |
p* |
R (95% CI) |
p* |
OR (95% CI) |
p* |
|
General obesity (BMI ≥ 30 kg/m2)† |
1.10 (0.62-1.93) |
0.7 |
1.65 (1.3-2.76) |
0.03 |
1.25 (0.92-1.86) |
0.3 |
Central obesity (WC ≥ 90 cm in men and ≥ 80 in women )† |
1.01 (0.56-1.82) |
0.5 |
1.2 (0.66-2.36) |
0.3 |
1.09 (0.82-2.96) |
0.4 |
Hypertriglyceridemia (TG ≥ 150 mg/dl)‡‡ |
1.11 (0.66-1.88) |
0.6 |
1.09 (0.72-1.65) |
0.6 |
1.10 (.80-1.52) |
0.5 |
Hypercholesterolemia (TC ≥ 200 mg/dl)‡‡ |
1.18 (0.69-2.04) |
0.5 |
1.06 (0.70-1.61) |
0.7 |
1.12 (.81-1.56) |
0.4 |
hyper-LDL cholesterolemia (LDL-C ≥ 160 mg/dl)‡‡ |
2.11 (1.18-3.76) |
0.01 |
0.97 (0.63-1.5) |
0.9 |
1.31 (0.93-1.85) |
0.1 |
hypo-HDL cholesterolemia (HDL-C < 40 mg/dl in men and < 50 in women)‡‡ |
2.72 (1.22-6.05) |
0.01 |
0.75 (0.45-1.25) |
0.2 |
- |
- |
| *P≤0.05 in multivariate regression model is considered as significant ‡Adjusted for age, physical activity, diabetes family history, smoking and energy intake, TG and TC ‡‡Adjusted for age, physical activity, family history of diabetes, alcohol consumption, smoking, BMI, antilipid medication, fiber intake and energy intake Table 3: Odds ratios (95%cofidence interval) for the associations of ApoB Ins/Del with risk of dyslipidemia and general and central obesity |
||||||




































