Open Access
Research Article
Max Screen >>
ISSN: 2393-9060
Copyright: © 2016 Rao S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background: As stunting in early postnatal life is prudent in developing countries, investigating its long term effect on adult blood pressure is necessary.
Methods: Young adults (males 449 & females 267) from rural cohort, who were also studied during their preschool age, were measured for anthropometry and blood pressure (systolic–SBP, Diastolic– DBP).
Results: Prevalence of overweight was low (5.6%) and that of obesity was negligible, but that for early life stunting (Z score<-2) was high. Stunting at 3+ yr affected significantly the adult measurements weight, height and leg height (p<0.00 for all) but not body mass index (BMI) or body fat (%). Prevalence of high blood pressure was significantly higher among males. Mean SBP and DBP increased significantly (p<0.01) from lower to higher tertile of adult BMI in both sexes. However, increase in the prevalence of high SBP (3.4% to 10.6%), high DBP (5.4% to 15.9%) and hypertension (8.1% to 22.5%) was significant (p<0.00) only among males. Further, the prevalence of high DBP was significantly higher among males stunted in early life. In particular, the risk of hypertension after adjusting for adult BMI (or body fat), was significantly higher (OR=2.8; CI: 1.2 - 6.4) among males who experienced stunting at 3+ yr compared to those who did not and was primarily due to significant risk for HDBP (OR=3.4; CI: 1.3 - 8.7).
Conclusion: Results highlight long term impact of stunting indicating developmental origins of hypertension and has implications for Asian population where stunting is predominant.
Keywords: Early life stunting; Hypertension; Young rural Indian adults
Though evidence about an inverse association between birth weight and adult blood pressure is now abundant [1], it is mostly from developed countries and little is known about it in developing countries [2] where a large proportion of children experience not only intrauterine fetal growth retardation but also postnatal retardation in early life. Studies linking birth length or ponderal index to adult blood pressure are few and those linking early postnatal growth are even scarce [3]. Since growth faltering in first two or three years of life is prudent in developing countries, its long term consequences may have strong impact on adult health in such populations.
The notion that exposures operating during childhood that influence growth are important in the etiology of coronary heart disease (CHD) has received attention of several researchers. Adult height trajectories are set early in childhood and early life conditions seem to affect adult height to a greater extent than the conditions in later childhood. A study from Guatemala [4] shows that prenatal and postnatal (first 2 years of life) nutritional influences are equally important in determining adult body size. But there are only few prospective studies with good measures of exposures across different stages of life course and with follow up to adult disease outcomes [5]. Nevertheless, it has been reported that poor childhood height growth may be associated with adult systolic blood pressure through socially patterned factors such as early nutrition, infection or stress [6]. These observations indicate that stunting in early postnatal life may also play a role in promoting chronic metabolic diseases in later life.
Identification of determinants of blood pressure in Asian people has an important societal implication. For, recent research suggests that association between blood pressure and stroke is stronger in Asian population and that reduction of 3 mmHg in diastolic blood pressure should reduce number of strokes in eastern Asia by one third [7]. Thus investigations on early postnatal growth and blood pressure are of high relevance, of high public health importance and may help to minimize adverse effects of disturbed fetal growth. Present study aims to examine the influence of stunting in early life on adult blood pressure in a rural Indian cohort.
Study subjects are the part of cohort spread over seven villages, situated at 40-50 km distance from Pune. These are the subjects who were studied for examining nutritional status in earlier projects conducted in 1979-81 during their preschool age i.e. 0 to 5 yrs, and were followed up in 1984-86 and then in 1988-93 during adolescent growth study giving data for the age group (8-18 yrs).
From the cohort who had completed 18 yrs age, 716 (66%) subjects (449 males and 267 females) could be located and were examined for anthropometric and clinical measurements during April 2003 to December 2005. Males were engaged either in cultivation in the same village or were in job outside the village. Most girls in the cohort had got married and were residing in various villages within the radius of 40-50 km outside their native village. As such it was very difficult to contact young married girls. However, with the help of local community worker from each village, initial work of contacting subjects, finding their convenient day and time of the week, actual surveys were planned.
Measurements were obtained according to standard techniques & were recorded by trained investigators in the earlier as well as in the current study. Weight (using digital electronic balance, least count 20 gm) & height (using stadiometer, upto 0.1 cm) were measured barefoot, in duplicate & average of two was used to calculate BMI (Kg/m2). Body fat was obtained using Omran’s electronic equipment (HBF-300). Age assessment was done in earlier projects on the basis of birth dates using school records and was once again confirmed at the time of current study. Ethical permission for the study was obtained from the Ethical Committee of Agharkar Research Institute and a written consent from each subject was taken.
A medical doctor was included in the survey team for measuring the blood pressure (using sphygmomanometer, Diamond Deluxe, India). Systolic (SBP) and diastolic (DBP) blood pressure was measured on the left hand in lying position after a rest of 10 minutes, and a duplicate reading was taken with a gap of 5 minutes between the two observations. Average of the two readings was used for analysis.
Hypertension was defined as blood pressure≥140/90 mmHg or if the subject was taking anti-hypertensive medication according to the report of JNC VII [8]. Thus high systolic blood pressure (HSBP) is defined when SBP≥140 mmHg and high diastolic blood pressure (HDBP) is defined when DBP≥90 mmHg. The prevalence of hypertension was computed including those on medication.
Since we had serial measurements on each subject during their preschool years Dugdales Growth Index [9] was calculated for weight (DUGW) as well as height (DUGH) to summarize the longitudinal information into a single index. In order to see the relative importance of age windows within first five years of life, the index was computed separately for subjects having observations during 0-1 yr, during 1-3 yr age and during 3-5 yr age. Based on this index, the prevalence of stunting (DUGH<90) or underweight (DUGW<80) was computed for respective age windows.
Mean values of various anthropometric measurements and blood pressure between stunted and non stunted group were tested using ‘t’ test. Differences in mean blood pressure levels by tertiles of BMI were tested using one way ANOVA and linearity test was done for examining trend. Logistic regression was performed to obtain odds ratios (OR) for risk of high blood pressure for subjects who were stunted at 3+ yr with considering non stunted group as reference category. ORs were adjusted for adult BMI or adult body fat (%) to examine independent effect of early life stunting. All the analysis was carried out using SPSS/PC+ 17.0 versions for windows.
The characteristics of young rural subjects in the study given in Table 1 show that rural subjects were thin (mean BMI of 20.3±2.9 kg/m2 for males and 19.4±2.8 kg/m2 for females) and short (mean height 166.3±6.1 cm in males and 152.7±5.6 cm in females) as adults. The prevalence of overweight was low in both the sexes (6.5% in males and 4.1% in females) while obesity was hardly present. In fact, a higher proportion of both males (29%) and females (43.4%) were undernourished (BMI<18.5 kg/m2 ). Mean values for almost all anthropometric measures were significantly higher for males compared to females except that for mean body fat (%). Similarly, mean blood pressure levels were significantly higher for males than females.
In pre-school years (0-5 yrs) of these subjects, prevalence of under nutrition was high (Table 2). Thus prevalence of stunting was 12.9% in males and 16.2% females during their infancy but increased significantly between 1-3 yrs age (47.1% in males & 43.2% in females) and remained high during 3-5 yrs, age especially among females (50.9% in males & 58.5% in females). Proportion of underweight was high even during infancy in both sexes and increased significantly beyond infancy.
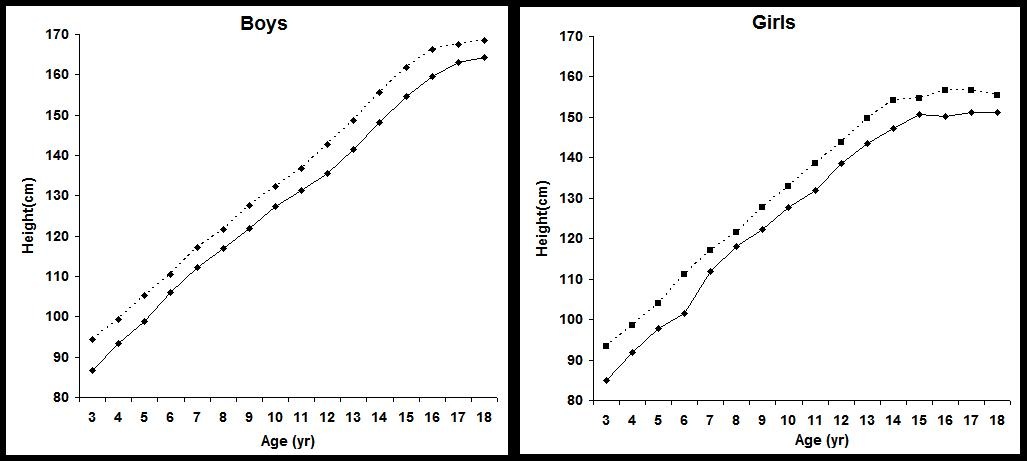
Mean adult height was significantly affected by early life stunting (Table 3). Thus subjects who were stunted during infancy had significantly (p<0.000) lower adult height (160.3±7.3 cm for males; 148.3±6.1 cm for females) compared to those who were not stunted (168.5±5.0 cm for males; 154.4±5.1cm for females). Stunting during infancy thus affects adult height by 8.2 cm in males and by 6.1 cm in females. However, the effect is reduced if stunting occurs during 1-3 yr age (4.2 cm in males and 5.4 cm in females) and sustains if stunting occurs during 3-5 yr age (4.8 cm in males and 5.2 cm in females). Adverse effect was also seen on adult sitting height and showed similar trends in both sexes. Thus, stunting at 3+ yr seems to have sustained effect on adult height and its components. However, it is worthwhile to note that there was no effect on adult BMI or adult body fat (%) in both the sexes.
We considered stunting at age of 3+ yrs using Z-score (<- 2) for height based on WHO (2006) standards to indicate early life stunting for further analysis. The entire growth curve from 3-18 yrs shows (Figure 1) that height at each age beyond 3+ yr, remains significantly low for the stunted group compared to those who were not stunted at 3+ yr.
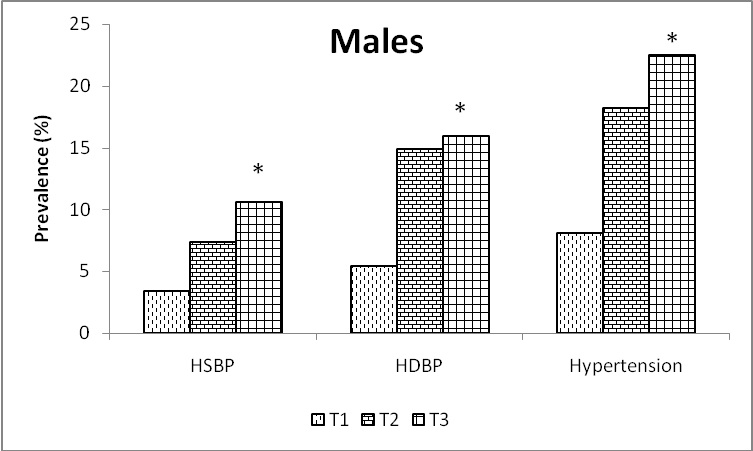
The prevalence of HSBP, HDBP and hypertension was significantly higher in males (7.1%, 12.0% & 16.2% respectively; p<0.00 for all) compared to that in females (1.9%, 4.5% & 6.4% respectively). The prevalence of HDBP was higher than that for HSBP in both sexes. Although the prevalence of overweight was small in both sexes, the adult BMI showed strong positive association with blood pressure levels. Thus, mean SBP levels increased significantly (p<0.000) from lower tertile of BMI to higher tertile both in males (116.5±10.4 mmHg to 123.1±11.1 mmHg) and females (109.4±9.2 to 114.8±9.4 mmHg). Similar increasing trends in mean DBP levels with increase in BMI from lower to higher tertile were also statistically significant (p<0.00). Prevalence of HSBP, HDBP and hypertension too increased from lower tertile to higher fertile of BMI and the trend was significant (P<0.00) for HDBP and hypertension, especially among males (Figure 2).
As stunting in preschool age of these subjects was considerably high, the prevalence of hypertension was computed within every tertile of adult BMI, separately for subjects who were stunted or not stunted at age 3+ yr (Table 4). Among males, prevalence of hypertension was marginally higher (p=0.07) in the highest tertile of BMI for subjects who were stunted in early life compared to those who were not. Separate analysis for HSBP and HDBP indicated that these trends were more prominent (P<0.05) in case of diastolic blood pressure than systolic blood pressure. Even in the lowest tertile of adult BMI, the prevalence of hypertension among stunted subjects was as high as 23.8% indicating the effect of early life stunting. In females too, the prevalence was higher among stunted compared to not stunted but the differences were not statistically significant.
Logistic regression analysis was done for computing risk of hypertension, HSBP and HDBP after adjusting for adult BMI or adult body fat percent (Table 5). It can be seen that, even after adjusting for adult BMI, stunting in early life in males shows significant risk for hypertension (OR- 2.7; CI: 1.2 – 6.2; p<0.05) and HDBP (OR- 3.25; CI: 1.27-8.3; p<0.05) but those in females are not statistically significant. These risks remained similar after adjusting for body fat (%) too.
Studies in different populations have demonstrated [10] an association of elevated blood pressure in adulthood with fetal growth (birth weight) or that with postnatal growth [3,11]. Associations of birth length or postnatal skeletal growth with adult blood pressure may be more important for planning appropriate strategies in populations where stunting is predominant in first few years of life. In rural Indian cohort, it was observed that stunting at 3+ yr not only affected adult height but additionally conferred significantly high risk for elevated diastolic blood pressure and hypertension in males even after adjusting for adult BMI or body fat.
Before discussing the results it may be worthwhile to discuss some of the following points. Though, we did not have data on birth weights, it cannot be overlooked that we have several serial measurements in preschool years for assessing postnatal undernutrition in early life and its effect on adult blood pressure. Secondly, it was not possible to have self monitored blood pressure to avoid white coat effect but is not a serious limitation as the subjects had familiarity with the investigators due to frequent follow up surveys and that the average of two readings was used in the analysis. Thirdly, we did not collect data on sodium intake, diet, life style factors or stress which are likely to influence blood pressure but are unlikely to negate the observed association between stunting and blood pressure.
The prevalence of overweight (BMI>25 kg/m2) among these young rural adults was negligible while that of undernutrition (BMI<18.5 kg/m2) was considerably high in both sexes. High prevalence of undernutrition in young rural adults from India is also reported by NFHS [12]. During preschool age of the subjects, proportion of stunting was small during infancy but increased substantially during 1-3 yr and remained high beyond 3+ yr especially among females. Number of studies [13,14] have reported peak prevalence of wasting and stunting around 2-3 yr, but have not examined the long lasting effect on adult height and its components based on longitudinal data.
Chronic malnutrition characterized by stunting remains a worldwide public health problem in spite of modest but consistent improvements in health status. Researchers [15,16] have shown that linear growth retardation increases risk for shortness in adulthood and results in low fat free mass. We too observed that subjects experiencing stunting in early life, especially at 3+ yr. had significant and sustained effect on adult height and components of height. The first 3 yrs of life are thus critical for their long term health implications. Chronic undernutrition hinders the growth potential of children and results in adults of low stature [17].
Although stunting has been described as an independent risk factor for the development of obesity, the relationship between stunting and obesity has been shown to vary due to differences in social and economic development in different populations [18]. In our study mean adult BMI or mean adult body fat (%) was not significantly different for those who were stunted in early life compared to those who were not. Similar results are also reported by Li H, et al. [4] in case of children from Guatemala. Our observations thus do not show that retardation in length during early childhood increases fatness in later life as reported by Victora CG, et al. [19].
The mean blood pressure levels observed for rural subjects were slightly lower than those reported for urban well nourished subjects [15]. Within the narrow range of BMI observed in this study, mean blood pressure levels were significantly positively associated with current nutritional status of the subjects. Thus, mean SBP for subjects in higher tertile of adult BMI was significantly higher compared to those in lower tertile (6.6 mmHg in males and 5.4 in mmHg females). Similar differences were observed for mean DBP levels too. A recent study by Mufunda, et al. [14] described a related finding where blood pressure positively correlated to BMI only in the normal range of BMI but the relationship ceased to exist at low or very high BMI. There is extensive heterogeneity regarding the relationship of BMI and blood pressure in different settings and more research is urgently required to unravel the intricacies of this relationship. However, the increasing trend in the prevalence of high DBP and hypertension from lower to higher tertile of adult BMI was significant only in males. Lack of such relationship has also been reported in case females from south India [16]. The non significant risk in case of females may indicate beneficial influence of estrogens. High prevalence of HDBP, in young rural adults with absence of obesity but presence of under nutrition in early postnatal life highlights the developmental origin of hypertension in this population. Similar observations are reported both in case of adolescents [23] and adults from India [24].
The fact that a large proportion of our subjects had experienced undernutrition in their early life draws attention to the role of postnatal nutritional status. Since growth is particularly intense in first two years of life, nutritional problems during this period may result in diverse manifestations, depending on the nature of the process. Thus, Mendez, et al. [25] have shown that children stunted between 0-2 yr had lower cognitive test scores than non-stunted while in a Jamaican study [26] children identified as growth retarded had increased response to psychological and physical stresses at 8-10 yr age. We observed that in every tertile of adult BMI, the prevalence of hypertension was higher among subjects stunted in early life compared to those not stunted. But with increase in adult BMI, the prevalence of hypertension increased by several fold among stunted females than stunted males. It may be recalled that extent of stunting in early life was more in females than males as stunting is the main risk factor probably with increase in adult BMI the effect is more pronounced in females than males. A study from Brazil [27] reports that women with short stature (<152 cm) had 3.08 fold greater risk of hypertension compared to those with normal height.
It has been suggested that inefficient endocrine control caused by reduced levels of insulin like growth factor-1 and /or altered expression of the hormone receptors that result from nutritional deprivation during early life, may exert negative influence on the general development of the individual and of the vascular system in particular, thus leading to an increased risk of hypertension. Barker DJ, et al. [28] too postulated that maternal undernutrition not only results in shorter length at birth but also responsible for changes in blood flow in several vascular beds reflecting alterations in vascular structure (viz. stiffness of arteries) and functions. Reduced elastin deposition further leads to ‘stiffer’ arteries and may result in raised blood pressure. These observations support our finding that the risk for high DBP was affected owing to early life stunting. A new explanation to possible mechanisms is offered by Wendy, et al. [29] in terms of reduced nephron numbers owing to intrauterine growth retardation as a risk factor for hypertension. These infants have smaller kidneys, whose circumferential dimensions are often more compromised than their length. Although, low birth weight is major health problem in rural India the possibility of smaller kidney size in our subjects could be a possibility but unfortunately have no data on either birth weight or kidney size.
In conclusion, a large proportion of young adults in rural India had experienced undernutrition in early life which had significant impact on adult height and its components i.e. leg height and sitting height. Further, our observation that prevalence of undernutrition stabilizes beyond 3+ yr and has its impact on adult size highlights the importance of critical window for correcting growth disturbances in such populations. Unfortunately, the existing nutrition intervention programs in India mostly cover children between 3-6 yr through kindergarten activities but miss large proportion of children in 0-3 yr age. Most importantly, early life stunting showed significantly high odds ratio for the risk of high DBP in males. It has been speculated that factors such as childhood diet, illness and psychosocial deprivation may through endocrine control, simultaneously influence growth of the arteries and of the bones at specific hormonally controlled phases of development leading to both short height and high blood pressure in adult life [30]. It is for this reason; the findings in this study indicate the influence of factors over and above the childhood exposures, perhaps pointing towards the developmental origins of hypertension. It is beyond doubt that policies for prevention of stunting among undernourished communities are essential to reduce the CVD risk during adulthood. Finally, as stunting is a major problem not only in India but also in Asia and other developing countries, the relationship of postnatal growth with CVD risk needs to be examined across different populations.
Evidence of validity of the newly developed KAP-HLQ has been obtained. This instrument can serve as an important tool to evaluate knowledge, attitude and practice on healthy lifestyle among Malaysian adolescents.The financial support was received from by Indian Council of Medical Research, New Delhi, India for carrying out this study. Author is grateful to the Director of the Agharkar Research Institute for providing facilities for this research. Author would also like to thank DR. Mrs. Kanade A N, Sayali Joshi, Kanchankumar Patil and other technical staff members in the department for their help in executing the project in the field. Thanks are also due to young rural subjects from the rural cohort for extending the necessary cooperation.

![]()

 |
 |
| Figure 1: Mean height between 3-18 yr for subjects stunted & not stunted at 3 yr |
 |
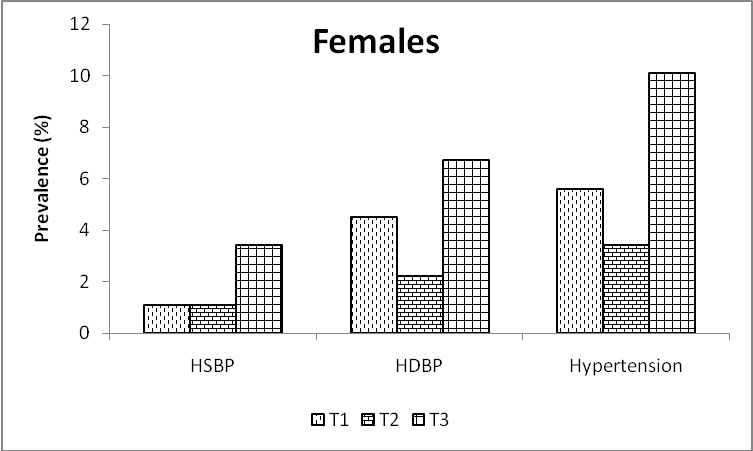 |
| *- p<0.05 for trend from lower to higher tertile BMI: Body mass index (Kg/m2) HSBP- systolic blood pressure >=140 mmHg HDBP- diastolic blood pressure >=90 mmHg Hypertension- either systolic blood pressure >=140 mmHg or diastolic blood pressure >=90 Figure 2: Prevalence of HSBP, HDBP and HYPT by tertiles of adult BMI among rural adults |
Parameters |
Males |
Females |
N |
449 |
267 |
Age (yr) |
23.2±2.6** |
22.9±2.7 |
Weight (Kg) |
56.2±9.1** |
45.4±7.9 |
Height (cm) |
166.3±6.1** |
152.7±5.6 |
BMI (Kg/m2) |
20.3±2.9** |
19.4±2.8 |
| % Overweight (BMI >=25 Kg/m2)
(BMI >=30 Kg/m2) |
6.5
0.2 |
4.1
0.7 |
% Underweight (BMI <18.5 Kg/m2) |
29.0 |
43.4 |
Body fat (%) |
15.7±5.4 |
21.0±6.2** |
Systolic blood pressure(mmHg) |
120.3±11.2** |
112.1±10. |
diastolic blood pressure(mmHg) |
76.3±9.3** |
73.0±8.2 |
| **: p<0.01 for sex differences BMI: Body mass index (Kg/m2) Table 1: Characteristics (mean ± sd) of young rural adults |
||
|
Males |
Females |
||||
|
Age (yr) |
N |
Underweight$ |
Stunted# |
N |
Underweight$ |
Stunted# |
0-1 |
101 |
30.7 |
12.9 |
68 |
39.7 |
16.2 |
1-3 |
240 |
57.1 |
47.1 |
148 |
58.8 |
43.2 |
3 -5 |
232 |
59.9 |
50.9 |
147 |
60.5 |
58.5 |
| $: Dugdale Growth Index for weight <80 in respective age groups #: Dugdale Growth Index for height <90 in respective age groups Table 2: Prevalence of underweight and stunting in early life |
||||||
Age (yr)
|
Early life nutrition Status | n |
Weight
(kg) |
Height (cm) | Sitting Ht (cm) | BMI (Kg/m2) | Body Fat (%) |
Males |
|||||||
0+ |
Stunted |
13 |
51.3±8.4 |
160.3±7.3 |
83.8±2.7 |
20.0±3.0 |
14.7±5.4 |
Not stunted |
88 |
56.3±9.0 |
168.5±5.0 |
87.1±3.1 |
19.8±2.7 |
13.9±4.7 |
|
p |
ns |
0.000 |
0.000 |
ns |
ns |
||
1-3 |
Stunted |
112 |
53.7±8.3 |
164.2±6.2 |
85.1±3.4 |
19.9±2.7 |
15.1±5.5 |
Not stunted |
127 |
57.4±9.4 |
168.4±5.8 |
86.8±3.2 |
20.3±2.9 |
15.7±5.0 |
|
p |
0.002 |
0.000 |
0.000 |
ns |
ns |
||
3-5 |
Stunted |
118 |
54.0±7.3 |
164.1±5.5 |
84.9±2.8 |
20.0±2.5 |
15.7±5.2 |
Not stunted |
114 |
59.1±10.0 |
168.9±5.9 |
87.1±3.2 |
207±3.2 |
16.1±5.3 |
|
p |
0.000 |
0.000 |
0.000 |
ns |
ns |
||
Females |
|||||||
| 0+ | Stunted | 11 | 41.5±8.3 | 148.3±6.1 | 76.1±3.6 | 18.7±2.5 | 19.4±5.9 |
| Not stunted | 57 | 45.5±7.9 | 154.4±5.1 | 79.9±2.6 | 19.0±2.8 | 20.4±6.4 | |
| p | Ns | 0.001 | 0.000 | ns | ns | ||
| 1-3 | Stunted | 64 | 44.4±7.5 | 150.1±4.8 | 78.1±3.0 | 19.6±2.7 | 20.9±5.7 |
| Not stunted | 84 | 46.9±7.0 | 155.5±4.2 | 80.4±2.8 | 19.4±2.7 | 21.3±6.2 | |
| p | 0.04 | 0.000 | 0.000 | ns | ns | ||
| 3-5 | Stunted | 86 | 43.0±7.1 | 150.2±5.4 | 77.9±3.1 | 19.0±2.7 | 19.9±5.8 |
| Not stunted | 61 | 48.0±8.9 | 155.4±5.3 | 80.4±3.0 | 19.8±3.2 | 21.9±6.9 | |
| p | 0.000 | 0.000 | 0.000 | ns | ns | ||
| $ - Dugdale Growth Index for height <90 in respective age groups BMI: Body mass index (Kg/m2) Table 3: Early life stunting$ & adult body size |
|||||||
Tertiles of adult BMI |
Males |
Females | ||
Stunted at age 3yr |
Not stunted |
Stunted at age 3 yr |
Not stunted |
|
Lower |
23.8 |
5.9 |
6.7 |
0 |
Middle |
22.6 |
12.5 |
3.8 |
9.1 |
Higher |
34.6 |
21.4 |
17.6 |
6.7 |
| +: z score is <-2 for height at age 3+ yr using WHO (2006) standards BMI: Body mass index (Kg/m2) Table 4: Prevalence (%) of hypertension by tertiles of adult BMI and stunting+ at age 3 yr |
||||
Risk for |
Adjusted for | Males |
Females |
||
Stunted |
Not stunted |
Stunted |
Not stunted |
||
Hypertension |
BMI |
2.7*
(1.2 – 6.2) |
1.0 |
2.8
(0.47 – 16.8) |
1.0 |
Body fat |
2.55*
(1.14 – 5.7) |
1.0 |
3.44
(0.52 – 23.0) |
1.0 |
|
HSBP |
BMI |
1.53 (0.49 – 4.8) |
1.0 |
3.29 (0.26 - 42) |
1.0 |
Body fat |
1.41 (0.46 - 4.3) |
1.0 |
3.88 (0.27 – 56.8) |
1.0 |
|
HDBP |
BMI |
3.25* (1.27 – 8.30) |
1.0 |
1.91 (0.18 – 19.7) |
1.0 |
Body fat |
3.0* (1.2 - 7.5) |
1.0 |
2.01 (0.2 – 21.1) |
1.0 |
|
| *- p<0.05, HSBP – systolic blood pressure >=140 mmHg, HDBP– diastolic blood pressure >=90 mmHg, BMI- body mass index (Kg/m2), Hypertension – either systolic blood pressure >=140 mmHg or diastolic blood pressure >=90 mmHg @ z score is <-2 for height at age 3+ yr using WHO (2006) standards Table 5: Odds Ratios (95% CI) for risk of HSBP & HDBP among subjects stunted@at 3+ yr |
|||||




































