Open Access
Research Article
Max Screen >>
ISSN: 2394-6520
Copyright: © 2021 Ariff S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Recombinant tumor necrosis factor -thymosin alpha 1 (TNF-T) has been used in Russian oncological practice for a number of years. Recently published studies on its safety, effectiveness, and influence on life quality allowed to perform Markov-based modeling of cost-effectiveness of TNF-T in a complex therapy of metastatic breast cancer. The analysis of the results showed that TNF-T associated with an increase of quality-adjusted life by 0.08 QALY. Incremental cost-effectiveness ratio (ICER) in the baseline scenario was below the willingness-to-pay threshold (1,072,000 RUB; net monetary benefit 68,000 RUB). 30% decrease of the price of the drug led to the decrease of ICER to 751,000 RUB and increase of NMB up to 92,000 RUB. Deterministic sensitivity analysis showed that ICER did not exceed the willingness-to-pay threshold in any scenario. The reduced price may also be associated with up to 145,000,000 RUB budget savings annually.
Keywords:Quality-Adjusted Life Years (QALY); Cost-Effectiveness Analysis; Increment Cost-Effectiveness Ratio (ICER); Net Monetary Benefit (NMB); Budget Impact Analysis; Immunotherapy; Metastatic Breast Cancer
In recent years, the survival rate of patients with metastatic breast cancer (MBC) increased due to the advances in specific antitumor therapy and supportive care [1]. A meta-analysis [2] of 15 studies on MBC (n=18,678) showed no increase of the survival rate between 1980 and 1990, whereas in 1990-2010 the median survival rate raised from 21 months (95% CI = 18-25) to 38 months (95% CI = 31-47). In 1990-2010, the survival rate grew from 32 to 57 months in case of estrogen receptor positive MBC, and from 14 to 33 months for ER-negative tumors. In eight studies on newly diagnosed cases of stage IV MBC, the survival rate increased from 20 to 31 months.
Because of a higher survival rate, improved tolerance to treatment, and appearance of many active drugs, most female patients with MBC in developed countries are now candidates for treatment with several lines of chemotherapy.
Reviews of clinical practice, e.g. in the United States, show that women with MBC receive 4-6 lines of chemotherapy in average, and eight or more different regimens of treatment in some cases. It is especially true for HER2-positive and hormone receptor-positive breast cancers, when tumor characteristics and effective treatment allow such approach. However, the influence of multiple lines of chemotherapy on the survival rate remains disputable [3]. EMBRACE study [4] demonstrated that new drugs often add only several weeks to the life expectancy in this group; on the other hand, chemotherapy of advanced breast cancer is also aimed to prevent cancer-related symptoms and to improve life quality.
In Russia, immunotherapeutic methods are often used to reduce the toxicity of chemotherapy. Bryuzgin VV and Platinskiy LV [5] noted that the best results of treatment of oncological diseases is achieved when traditional approach is combined with cytokine therapy, which reduces the negative impact of chemotherapy on immunity and reduces the toxicity of some antitumor drugs. Russian researchers developed Refnot (recombinant tumor necrosis factor -thymosin alpha 1, TNF-T), a hybrid molecule of two biologically active agents, i.e. tumor necrosis factor (TNF) cytokine and thymosin hormone [5]. The drug is indicated for patients, who undergo complex therapy of breast cancer that include chemotherapy. A large-scale medical and sociological study published in 2016 demonstrated that the inclusion of TNF-T into the treatment of oncological patients improves their quality of life [6].
The present study was based on the data on the changes in life quality from that study with specific aim to evaluate effects in women with MBC. Its aim was to perform a cost-effectiveness analysis of TNF-T as an additional therapy in women with metastatic breast cancer, who received several lines of chemotherapy, and to perform budget impact analysis of widespread use of TNF-T in the therapy of MBC, if the price of the drug was registered or reduced. The analysis is driven by the attempt to limit toxicity of chemotherapy by using TNF-T while demonstrating favorable changes to quality of life and absence of large additional resources consumption.
A literature search in the Russian Science Citation Index (eLIBRARY.RU) bibliographic database resulted in 45 publications on the studied drug. Model studies on cells and laboratory animals, and conference abstracts were excluded. It was established that most publications considered Refnot in the neoadjuvant therapy setting [7-9], whereas the developed model assumed the use of the drug when surgical treatment of metastatic breast cancer is not possible. Therefore, the data on the change in prevalence of adverse events of chemotherapy were taken from these publications.
To analyze cost-effectiveness, a Markov model was created that included three states, i.e. no progression in treated patients, disease progression, and death. The Markov model was selected to address challenges with relative shortness of clinical trial and necessity to capture TNF-T effects during lifespan of women with MBC. There were no detailed data in Russian studies on the survival rate of patients, who received TNF-T in addition to chemotherapy. Instead, the data from the control group in EMBRACE study [4] were used in the model, because these patients better corresponded to the target population of patients, to whom TNF-T was to be administered in the present study. The inclusion criteria in EMBRACE were two or more chemotherapy regimens for advanced breast cancer; however, the actual number of regimens received by the participants before the inclusion was much higher (median 4 regimens).
As it was noted above, new drugs improved the survival rate of women with MBC. Therefore, it was decided to adjust the probability of survival with the data from control groups in more recent studies. It was assumed that the distribution of progression-free survival and overall survival was exponential. Data and charts from PALOMA-1 study [10] were used to assess the overall survival; it was possible to establish the time of survival of 80% patients including the control group. Parameters of distribution were based on this information.
The baseline scenario assumed that the administration of TNF-T only influenced life quality and not the duration of progression-free period. It was then assumed that the quality of life was 0.590 in the group that did not receive TNF-T, and 0.496 after the progression of the disease (the quality of life after the progression, when the use of modern drugs is no longer possible [11].
A large-scale medical and social survey of 336 oncological patients showed that TNF-T improves the quality of life [6]. It was necessary to include these changes into the model. According to the survey, 48.6% of the participants noted symptomatic relief, global health functioning improved in 20.5%, work capacity improved in 20.5%, physical functioning increased in 18.9%, and social and emotional functioning increased in 13.5% of the participants. These data were then translated into utility values as follows. Average values on EORTC QLQ-30 scales that are perceived by patients as changes (transition from one state to another) were taken from a study on breast cancer by Osdoba et al. [12]. These changes were translated into values based on EORTC QLQ-30 Scoring Manual [13], and utilities were calculated using weighting factors from a study by Marriott et al. [14]. Three domains of EORTC-QLQ30 were used (physical functioning, emotional functioning, and global health status). The obtained components of utility changes were multiplied by the share of patients, who noted improvements in a respective domain after the administration of TNF-T. The total life quality improvement was 0.035 in the units of utility.
For sensitivity analysis, an approach based on possible changes in EQ-5D questionnaire was chosen [15]. It was assumed that the patients, who noted improved physical functioning, would also note such improvement by at least one position of EQ-5D questionnaire. Improvements in social and emotional functioning were equated to the change by one position in the anxiety/depression domain of EQ-5D. Separate calculations of utility changes were performed for transitions from level 2 to level 1, and from level 3 to level 2. For the final evaluation, it was assumed that level 2 is two times more probable than level 3. The improvement of life quality was 0.044 in utility units according to this method.
It was also necessary to consider the decrease of life quality due to adverse effects of chemotherapy [7]. To do this, weighting coefficients from a study by Lloyd et al. were taken [16]. The decrease in life quality associated with non-febrile neutropenia was assumed to be similar to such in febrile neutropenia. The coefficient of life quality decrease due to adverse events, which were not analyzed in Lloyd et al. [16], was calculated as an average of six events considered in this study (febrile neutropenia, weakness, stomatitis, nausea and diarrhea, hair loss, and hand-foot syndrome (palmar-plantar erythrodysaesthesia). A total value was calculated as a weighted average. The overall life quality decrease was -0.077 in the control group and -0.056 in the group that received TNF-T as an addition to chemotherapy.
In was assumed that all patients receive chemotherapy. The costs of therapy was taken from the General Tariff Agreement for Saint Petersburg in 2018 (49,984.20 RUB for the code ‘ONС Malignant mammary neoplasms I-IV stage (chemotherapy)’, and 73,300.00 RUB for the code ‘Stage IV breast cancer (with bones metastasis etc.)’. The first value was included into the model.
The cost of therapy with TNF-T was calculated from the value in the state register of maximum sale prices (9,000 RUB for a pack of 5 flasks). It was assumed that the course included six packs, so the total cost of therapy was 54,000 RUB. Incremental cost-effectiveness was considered in the sensitivity analysis for 30% reduction of the registered price, which could be expected after the inclusion of TNF-T to the system of state purchases in the framework of free medical care for diagnosis-related groups (DRGs). The main indicator was quality-adjusted incremental cost-effectiveness in RUB per life year.
The horizon of the model was the end of life of the members of a hypothetical cohort. All analyzed costs were discounted at 3% per year. Sensitivity analysis was performed for two approaches to the estimation of life quality change and for the reduction of the cost of the drug.
Deterministic sensitivity analysis also addressed the influence of discount rate changes (from 0% to 5%) on the incremental cost-effectiveness, and the possible influence of the drug on the improvement of progression-free survival and overall survival [8,9].
Because article is based on aggregate data from clinical trial no IRB review was necessary
Both Markov modeling and sensitivity analysis were performed with R package heemod [17] for Windows (version 3.3).
The main results of the analysis of the baseline scenario and sensitivity analysis are shown in Table 1.
The analysis of the model showed that the total increase was about 0.08 QALY or about one quality-adjusted month of life. In comparison, the median QALY increase was 0.66 for main positions of the restrictive lists of antitumor drugs (not additional complex therapy) according to an analysis of 2014-2015 records performed by Kolbin AS et al. [18]. The data on the increase of quality-adjusted life allowed evaluation of net monetary benefit that includes the threshold of society’s willingness to pay for a quality-adjusted life year, and the costs of an evaluated medical technology. In this case, the net monetary benefit was over 65,000 RUB per patient with currently registered prices, and up to 92,000-94,000 RUB, if the cost of TNF-T reduced by 30%.
The difference in costs in case of addition of TNF-T to chemotherapy regimen indicates that most patients would receive little more than one course of therapy.
The Table shows that the cost of one quality-adjusted life year is about 1,073,000 RUB in the baseline scenario. If cost of novel medical technology is high, it usually compared to the willingness-to-pay threshold. Russian experts most often propose to use triple GDP per capita as a threshold [19,20]. In 2017, GDP per capita in the Russian Federation was 626,968 RUB, and the triple GDP per capita was 1.88 million RUB. The comparison shows that the modeled ICER values in both baseline scenario analysis and sensitivity analysis do not exceed the willingness-to-pay threshold. When GDP per capita is compared, it is sometimes proposed to divide interventions into highly effective (less than one GDP per one QALY), effective (less than three GDP per capita for one QALY) and ineffective (over three GDPs per capita for one QALY). It seems that the administration of TNF-T in a complex therapy of MBC can be considered an effective intervention.
In the already mentioned study by Kolbin AS et al. [18], the median incremental cost-effectiveness ratio of antitumor drugs included into restrictive lists was 2.5 million RUB for one QALY, and in one case it was over 10 million RUB for one QALY.
An analysis of deterministic univariate sensitivity was performed for a more detailed understanding of the influence of changes of initial conditions on cost-effectiveness. Its results are shown in Figure 1.
The Figure demonstrates that the incremental cost-effectiveness does not exceed the willingness to pay threshold with any considered changes of initial parameters. As it was expected, a decrease of the cost of TNF-T and of the discount rate led to a decrease of ICER. The parameters of overall survival had almost no influence on the cost-effectiveness because the model did not assume long-term decreased mortality of patients. It is worth noting that ICER increases along with the decrease of the progression-free survival. This can imply that the increase of costs due to repeated courses of TNF-T cannot fully compensate changes in life quality. At the same time, even a very optimistic assumption about the influence on the progression-free survival (RR=0.72 calculated from the results by Gaysina YA et al. [9] does not result in ICER values higher or even approaching the threshold of willingness to pay for the new medical technology.
For unbiased consideration of the importance of funding of therapy from budgets of various level and other issues, it is necessary to estimate the number of patients, who need this treatment. Unfortunately, no information on the actual use of TNF-T in Russian patients with MBC was found in the available literature. The number of cases of stage IV MBC was considered as a surrogate parameter for the number of patients, who may need this therapy; it was assumed that this entire group would ultimately need advanced lines of therapy. The data on the distribution of stage IV breast cancer were obtained as follows. A total number of newly diagnosed cases of MBC was found in Malignant Neoplasms in Russia in 2017 (Morbidity and Mortality) [21], and the data on the share of MBC were taken from The Condition of Cancer Care for the Russian Population in 2017 [22]. The absolute number of MBC cases was calculated by multiplication of these two parameters. The analysis of the data from 2007-2017 showed that the number of cases of MBC was 5,500-5,600 cases annually, and now it has a growing trend after some decrease in 2007-2011; linear regression coefficient was 47, i.e. increment is lower than per one hundred cases. The use of TNF-T in all these patients would require 482,700,000 RUB per year in current prices without a discount, or 337,900,000 RUB if the prices would be reduced by one third. In real-life conditions, however, the costs should be lower because far from all women would be treated with this drug. Also, it should be noted that the drug is already included into the list of vital and essential drugs and therefore it should be provided to patients in hospitals out of budgetary funds. In this respect, a new, lower registered price could lead to budget savings of up to 144,800,000 RUB per year.
It should be taken into account that present study based on results of one large-scale study of TNF-T and some might have limited generalizability. Also it used cross-walk from questionnaires used in the study to the utilities and in future studies it would wise to include standard instruments like EQ-5D in the Protocol.
In general, it can be concluded that TNF-T increases the quality of life of female patients with MBC, which reflects on its cost-effectiveness. The cost of one added year of life is under the threshold of willingness to pay for a new medical technology both in baseline scenario and in all sensitivity analyses performed. If TNF-T will be used in complex therapy of MBC in women, who already received other treatment possibilities, and if its price will be registered, the budgetary expenses may be reduced by up to 145,000,000 RUB annually.

![]()

Source of utility values |
Difference in total costs, RUB |
Difference in QALY |
ICER, RUB/ QALY |
NMB, RUB |
EORTC-QLQ30 |
87518 |
0.0816 |
1072744 |
65932 |
EQ-5D |
87518 |
0.0828 |
1057619 |
68127 |
EORTC-QLQ30 |
61263* |
0.0816 |
750925 |
92187 |
EQ-5D |
61263* |
0.0828 |
740338 |
94382 |
*30% reduction of the cost of TNF-T; QALY: Quality-Adjusted Life Years, ICER: Incremental Cost-Effectiveness Ratio in Rub Per a Quality-Adjusted Life Year; NMB: Net Monetary Benefit
Table 1: The results of the baseline scenario analysis (bold) and sensitivity analysis of the cost-effectiveness of TNF-T in complex therapy of MBC
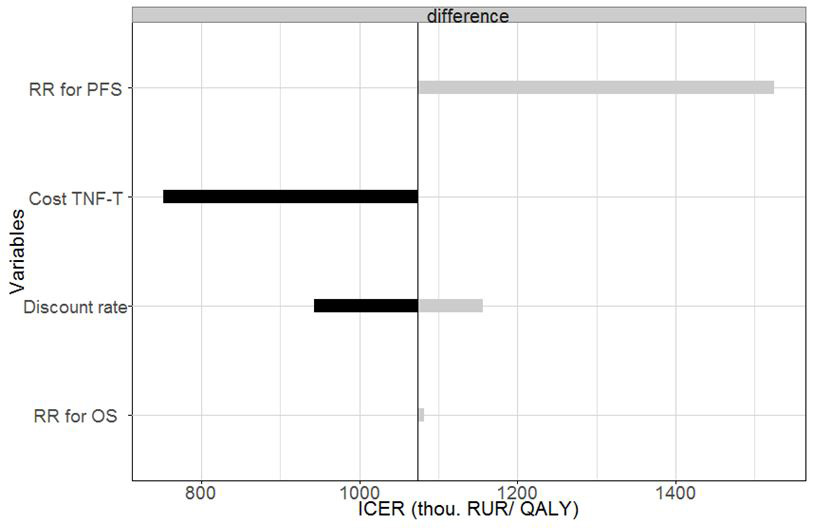 |
Figure 1: The results of sensitivity analysis. RR: Relative Risk; OS: Overall Survival; PFS: Progression-Free Survival. Vertical line shows ICER values in baseline scenario |




































