Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2016 El Ansari R. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Introduction: Neuroendocrine neoplasms are defined as epithelial neoplasms with predominant neuroendocrine differentiation. They are most commonly found in the gastrointestinal tract and respiratory system. Nasal cavity and paranasal sinuses are a rare site for neuroendocrine carcinoma; it’s reported as a recurrent entity and locally destructive tumor.
Very few cases of paranasal sinus neuroendocrine carcinoma have been reported till date.
We report one such case and discuss the specificities of this location.
The paper represents recent treatment trends that may result in improved loco regional control and survival
Case report: We report the case of 42-year-old women without known pathological history, who presented with bilateral nasal obstruction with purulent rhinorrhea since 2 months. Diagnosis was made on the basis of immunohistochemical study of biopsy samples. Treatment, comprising chemotherapy followed by radiotherapy, achieved total remission at 9 months follow-up.
Discussion/Conclusion: Neuroendocrine neoplasms are rare. Diagnosis is based on immunophenotypic and molecular characteristics. It is an aggressive neoplasm, requiring multidisciplinary management.
Keywords: Nasal cavity; Paranasal sinuses; Neuroendocrine carcinoma; Small cell carcinoma
Within the head and neck region, neuroendocrine carcinoma (NEC) is most commonly found in the larynx, followed by the salivary glands [1]. It is very rarely found in the nasal cavity and the paranasal sinuses, accounting for approximately 5% of malignancies at these sites [2]. It is classified into well-differentiated (typical carcinoid), moderately differentiated (atypical carcinoid), and poorly differentiated neuroendocrine carcinomas.
The last category is further subdivided into small cell and large cell variants.
Very few cases of paranasal sinus neuroendocrine carcinoma have been reported till date and no therapeutic protocol has been adopted.We report one such case and discusses the specificities of this location. The paper represents recent Treatment trends that may result in improved loco regional control and survival,
42-year-old women without known pathological history presented with bilateral nasal obstruction of progressive onset, associated with fetid bilateral purulent rhinorrhea and upper dysphagia of 2 months evolution in a context of apyrexia and 4 kg weight-loss over 3 months.
ENT examination found a fleshy burgeoning polypoid formation, bleeding on contact and filling the entire right nasal cavity, pushing back the ipsilateral middle turbinate and nasal septum. Endoscopy was impossible due to the size of the mass. Otherwise, clinical examination, notably of the lymph-node regions, was normal.
Bacteriological examination of the secretions, sampled by direct swabbing of the nasal cavities, was negative. Sinonasal CT found filling of the maxillary and ethmoid sinuses with lysis of the medial wall of the right maxillary sinus extending into right nasal cavity causing erosion of nasal septum (Figure 1). Magnetic resonance imaging showed a heterogeneous filling of paranasal sinus without intracranial or orbital extension (Figure 2). Histopathologic analysis biopsy from nasal mass found a widely ulcerated cylindrical coating.
Immunohistochemistry (IHC) revealed that neoplastic cells were positive for cytokeratin, Anti Ki67, synaptophysin, and chromogranin and negative for S-100. Mitotic count was 30–40/10hpf. A diagnosis of poorly differentiated neuroendocrine carcinoma with small cell (SNEC) of paranasal sinus was reported.
Extension assessment, comprising chest X-ray, thoracic-abdominal-pelvic CT, was negative.
Treatment consisted in adjuvant polychemotherapy, with six cycles (cisplatin and etoposide), There was gross reduction in tumor volume. Followed by loco regional external radiotherapy (paranasal sinus and nasal cavities: 48.6 GY in 35 sessions).
After one year follow-up, the patient was in complete clinical and radiological remission (Figure 3a, b and c) and the rhinoscopic control found an inflammatory nasal mucosa without histologic malignancy.
SNEC of the nasal and paranasal cavities has demonstrated aggressive clinical behavior and a poor prognosis, with fast tumor expansion, early local recurrence, and widespread dissemination [3,4].
SNEC is a rare entity, accounting for 5% of all tumors in the sinonasal region; it has demonstrated aggressive clinical behavior and a poor prognosis, with fast tumor expansion, early local recurrence, and widespread dissemination [5]. Moreover, Less than 270 cases of head and neck SNEC have been published until 2006 March including 69 cases of SNEC in nasal and paranasal sinuses in the world literature [6,7].
SNEC in paranasal sinuses has been described to affect primarily adults without gender differences [8]. The average age of incidence is about 41.5 to 55.0 years old (10 to 79 years), and the common sites of SNEC are ethmoid sinus and maxillary sinus [9].
A strong linkage with smoking has not been identifie and any corelation between EBV infection and occurrence of sinonasal Neuroendocrinecarcinoma [10].
Clinical presentations include nasal obstruction, epistaxis, and facial mass or facial pain [11]. The most frequent sites for distant metastases are the lungs, liver, and bone [12].
Radiological examination is important to determine the hallmarks of the local tumor invasion (Bony erosion on CT and intermediate signal intensity on T 2 on MRI), and are better for the planning of further treatment [12,13].
The treatment of sinonasal neuroendocrine carcinomas has not been systematically evaluated because of small number of cases. No agreement for adequate management has been reached among oncologists, and some recommendations have been developed from retrospective data [14].
Surgery, radiotherapy, or chemotherapy therapeutic methods both alone or in combinations are used by various head and neck oncologists. A group of oncologists favored surgery followed by radiotherapy [14].
However, more recent studies have claimed that neoadjuvant chemotherapy with cisplatin and etoposide and high-dose proton-photon radiotherapy is a successful treatment approach for SNEC patients in paranasal sinuses [13-15].
The paranasal sinus neuroendocrine tumors are recurrent and locally destructive. Multimodality treatment approach is needed. Even with multimodality treatment, local and distant recurrence is very high. Platinum-based chemotherapy followed by radiotherapy has shown promising results in treatment of poorly differentiated small cell neuroendocrine car-cinomas involving sinonasal tract. Recent treatment modality incorporating surgery as initial treatment followed by postoperative chemoradiotherapy is associated with better disease control and overall survival in treatment of sinonasal neuroendocrine carcinoma even in poorly differentiated small cell neuroendocrine carcinoma; however as majority of patients have advanced disease at presentation with extensive involvement of orbit, skull, and brain, surgical resection is usually difficult.

![]()

 |
Figure 1: Computed tomography (CT) of paranasal sinuses showing mass occupying the entire right maxillary and ethmoid sinuses extending into right nasal cavity causing erosion of nasal septum ( |
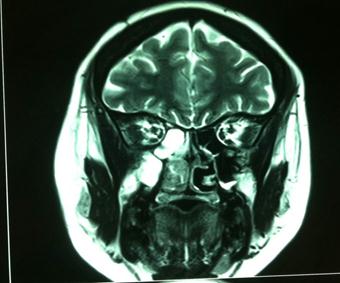 |
Figure 2: Magnetic resonance imaging showed a heterogeneous filling of paranasal sinus without intracranial or orbital extension |
   |
Figure 3: The post-treatment figures; (A) Complete tumor reduction in nasopharyngonasal cavity; (B-C) Gross reduction in tumor volume |




































