Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2016 Souldi H. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Teratoma of the nasopharynx is a very rare lesion with a high mortality rate due to severe airway obstruction, especially in the neonatal period. We report the case of a newborn child who presented with an inspiratory distress and apneic episodes due to a mass in the nasopharynx. Preoperative evaluation and imaging showed a solid-cyctic nasopharyngeal mass without intracranial extension. The swelling was excised surgically under general anesthesia. Histopathological examination showed an immature teratoma of the nasopharynx. The postoperative course was uneventful. Teratomas of the nasopharynx are rare and are treated by surgical excision. If respiratory distress accompanies the lesion, priority must be given to securing the airway. Early diagnosis and particularly prenatal diagnosis has greatly improved their prognosis.
Keywords: Teratoma; Nasopharynx; Neonate; Airway Obstruction
Teratomas are benign tumors containing cells from ectodermal, mesodermal and endodermal layers [1]. They may originate anywhere along the midline. The sacrococcygeal area is the most common site of extra-gonadal teratomas [2]. Teratomas of the head and neck are relatively rare. In the literature, less than 300 cases of neonatal head and neck teratomas were reported; most of them were of a cervical location. Teratoma of the nasopharynx is an extremely rare tumor; although usually of a benign histopathological nature, it may be life-threatening. Teratoma of the nasopharynx represents one of the most unusual causes of respiratory distress during the neonatal period [1,3].
Airway problems in newborn babies present a diagnostic difficulty. Relief of the obstruction must be as rapid as possible and diagnostic procedures must be performed speedily. Imaging studies are useful to show the location and extent of the nasopharyngeal teratoma and to aid in its clinical management [4]. The prognosis of nasopharyngeal teratoma has greatly improved by early diagnosis, particularly prenatal diagnosis and Ex-utero Intrapartum Treatments (EXIT procedures).
In this report, we present a case of a 30 d old child presenting a neonatal breathing difficulty due to nasopharyngeal teratoma treated by surgical removal and summarize a review of the literature on teratomas of the nasopharynx.
Thirty days old male infant delivered normally and appeared well at birth. He presented inspiratory distress during the first day of life. He was referred to our department for a clinical presentation of nasal obstruction, bilateral purulent nasal discharge, snoring, and apneic episodes during feeding since birth.
At initial examination, the patient had normal vital signs and exhibited no abnormalities on oropharyngeal examination and otoscopy. No congenital malformation was detected. Flexible nasofibroscopy showed a pedunculated nasopharyngeal mass arising from the superior nasopharyngeal wall, almost completely obstructing the choanes of both nasal cavities. The computed tomography with contrast injection was asked before the MRI for accessibility reasons. It showed a solid-cystic mass at the base of the skull measuring 19x16x15 mm and obstructing the choanes, other neighboring anatomical structures were normal (Figure 1). MRI with gadolinium injection was then performed on the one hand to guide the diagnosis of tumor types, on the other hand to consider its extension to the skull base and guide the process of excision. It did not show any relation with the intracranium or the large blood vessels in the neck (Figure 2).
Under general anesthesia, the tumor was excised completely utilizing an endoscopic surgical approach. There was no evidence of a cerebrospinal fluid leak. The patient’s clinical course improved in the immediate postoperative period. The histopathological examination of the specimen showed immature teratoma; histological analysis showed fibro connective tissue, neuroglia tissue and a squamous cell layer; there were no signs of malignancy.
Teratomas are embryonal neoplasms derived from pluripotent cells from all three primordial germ-cell layers: ectoderm, mesoderm and endoderm [5]. They occur in 1 out of 4000 live births [1]. Teratomas of the head and neck region account for about 5% of all reported teratomas. Most of them are located in the cervical region. Nasopharyngeal teratomas occur more rarely, they form only a small proportion of head and neck teratomas [2]. Despite female predominance of teratomas, there is no gender preference for those affecting the head and neck zone [6,7].
The most widely accepted terminology describes four types of teratomas: dermoid cysts (epithelial lined with skin elements, composed of ectodermal and mesodermal cells), teratoid cysts (all 3 germ layers but poorly differentiated), true teratoma (3 germ layers differentiated into specific tissues or organs), and epignathi (oral tumors with develop-mental fetal organs and limbs) [1]. Dermoid cysts comprise the vast majority [8]. Teratomas are divided into two groups: mature and imma¬ture. Mature teratomas include only adult tissues of the same age as the subject, unlike immature ones [5]. Approximately 20% to 40% of childhood teratomas contain some immature tissues. In childhood, 75% to 85% of teratomas of the head and neck region usually contain neuroectodermal elements (both mature and immature) such as our case [9].
The exact pathogenesis and origin of teratomas in the head and neck is controversial and various theories are suggested. One theory suggests that failure of fusion of midline structures during embryogenesis leads to a midline nasopharyngeal teratoma and cleft palate. Another theory postulates that they arise from uncontrolled growth of a misplaced pluripotent cells originating in the region of the embryonic notochord [10,11].
Symptoms of teratoma of the nasopharynx are dependent on the size and location of the lesion. Typically, it induces obstruction of the proximal ororespiratory tract, which requires rapid airway management especially in the neonatal period [3,6,8]. Dyspnea, failure to thrive, difficulty in feeding, or even intermittent symptoms of cough, cyanosis and dysphagia have also been reported [2]. They have an 18% risk of other congenital malformations [7], palatal fissures are common [7,8], hemicranias, anencephaly, cardiac abnormalities and atresia of the left common carotid have been reported [5,8,12].
Ultrasonography allows some of these tumors to be diagnosed prenatally [5,9,13]. Maternal serum alpha foeto-protein levels may be elevated [5,8,13]. Main circumstances of detection (20 to 50% of cases) are viewing the presence of a cervical or nasopharyngeal mass with solid and liquid components and polyhydramnios due to impaired swallowing [3,5,8].
Complications include stillbirth, prematurity, abnormal presentation and dystocia [5,6].
Management of the fetus with head and neck teratoma that threatens the airway remains a clinical challenge. This has been revolutionized by the use of Ex-utero Intrapartum Treatments (EXIT procedures) and the availability of fetal MRI that allows for a more accurate assessment of the airway prior to birth [14]. EXIT procedures are employed in the delivery of fetuses with large head and neck masses to obtain a stable airway while the newborn is maintained on utero-placental circulation. It allows avoiding airway obstruction, hypoxia and brain injury at the time of delivery by maintaining the uteroplacental gas exchange. EXIT procedure provides time to secure an airway, converting an emergent crisis into a controlled event. This may involve a combination of laryngoscopy, bronchoscopy, tracheostomy and tumor resection on placental support [14].
Preoperative CT and MRI may be helpful in making a diagnosis by the pattern of imaging density caused by the mixed tissue types [3]; teratoma appears as a heterogeneous formation on MRI [5] with intratumoral calcifications on CT [8]. In addition, imaging studies show the location and extent of the lesion, its relationship with vascular, bony and visceral structures, thus aid in the clinical management and the surgical approach [2,4,5]. In our case, there was no evidence of intracranial involvement.
The differential diagnosis of nasopharyngeal tumors in infants includes craniopharyngiomas, chordomas, hamartomas, encephaloceles, cystic lymphangioma, rhabdomyosarcoma, lymphoma neurofibromatosis and gliomas [1,5,8,12]. A meningoencephalocoele has continuation through a bony defect, with intracranial structures and cerebrospinal-fluid-dense areas within.
Nasopharyngeal teratomas are an otolaryngology emergency in terms of localization and clinical picture especially in newborns. Their treatment consists of surgical excision. These tumors are often encapsulated or pseudoencapsulated and not infiltrating, which facilitates dissection of the teratoma from surrounding tissue structures [2]. When a neonate is experiencing respiratory difficulty, the first priority should be stabilization of the airway [5,9,13]. If necessary, a tracheostomy has to be performed [3,10]. Before treating any congenital pharyngeal mass the surgeon must ensure that the mass has no relationship to vascular structures in the neck and does not have an intracranial extension or communication [3]. If there is any doubt, needle aspiration to exclude the presence of cerebrospinal fluid must be performed [7,8]. Although the complete extirpation is the ultimate goal of the treatment for head and neck teratomas, the surgical excision may be laborious and incomplete because of the complexity of the lesion and its extension into the surrounding structures in the complex anatomical area like nasopharynx. Hwang and al [15] describes the novel technique of radiofrequency coblation in the management of a congenital nasopharyngeal teratoma. The tumor was debulked with radiofrequency coblation from the center of the lesion, creating an overall effect of the tumor collapsing on itself. This method did not require extensive dissection of tissue planes and minimized intraoperative blood loss.
No cases of recurrence of teratoma after complete removal have been reported. Unlike adults, teratomas in children are often congenital and very rarely turn malignant. Malignancy is not equated with the degree of immaturity of the tissue elements. This case had no histological evidence of malignancy. It has been reported that immaturity of various constituent tissues in childhood teratomas (unlike adult) does not impact on the otherwise favorable prognosis of the teratoma [2,7]. Death in neonates usually results from respiratory obstruction due to lesion bulk and location [9,10], in contrast with the high mortality rate in the adult group which is due to high rate of malignant transformation.
Teratomas of the head and neck are often benign but they can potentially cause fatal airway obstruction. Surgical removal gives a complete cure. Close collaboration between radiologists, obstetricians, neonatologists, anesthetists, otolaryngologists and pediatrician is essential to achieve a prenatal diagnosis and program post-natal care to improve perinatal outcome.

![]()

 |
| Figure 1: Axial Section Computed Tomography Scan showing a solido-cystic mass at the base of the skull obstructing the choanes |
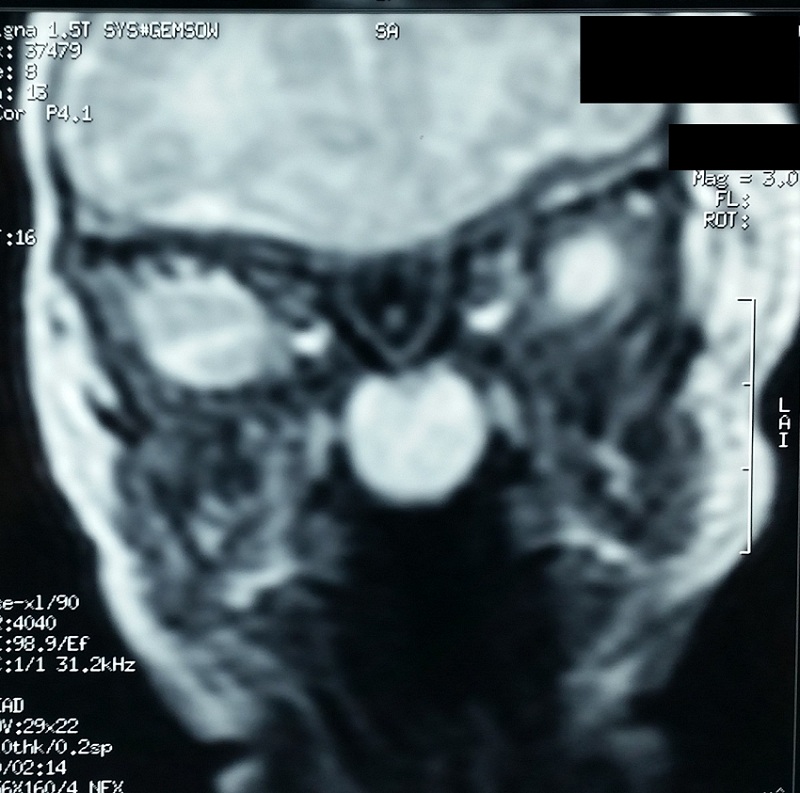 |
| Figure 2: Coronal T2-weighted MRI scan showing a heterogeneously soft tissue mass arising from the superior wall of the nasopharynx without intracranial extension |




































