Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2014 Rakhi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Appendicitis is a rare pregnancy associated surgical emergency, with appendectomy as the most frequent non obstetrical surgical procedure performed in pregnancy. Diagnostic delay increases maternal and fetal morbidity and mortality thereby highlighting the need for a prompt diagnosis and surgery. Two cases of appendicitis with pregnancy are being reported with abdominal pain as common presenting feature. One of these patients had fatal outcome probably due to delayed presentation, the other, however, was successfully managed with early surgical intervention leading to normal maternal and fetal outcome. Early surgical intervention in such cases merely on the basis of high index of suspicion is being emphasized.
Keywords: Appendicitis; Appendectomy; Pain; Pregnancy; Perforation; Mortality
Appendicitis is the inflammation of appendix, rarely associated with pregnancy with an estimated frequency of one per fifteen hundred pregnancies [1,2]. Appendectomy is a most common non obstetrical surgical procedure in a pregnant patient [1]. The accurate diagnosis of acute appendicitis in pregnancy is usually obscured due to gestational physiological changes. Delay in diagnosis enhances risk of appendiceal perforation, hence rising maternal and fetal morbidity and mortality. Symptoms and signs of appendicitis in pregnancy are quite enigmatic as they often vary with the varying trimester of pregnancy due to changing anatomical location of appendix with consequent enlargement of uterus. Appendicitis occurs most commonly in the first and second trimester but can occur at any gestation [1]. Here we are presenting two cases of acute appendicitis with pregnancy, out of which 1 patient died.
A 26-years old pregnant lady with previous one abortion was hospitalized at 34 weeks period of gestation with abdominal pain, vomitings and fever for last 24 hours. It was a generalized abdominal pain, more in the epigastrium. On examination, she was febrile but hemodynamically stable. She had epigastric abdominal distension and tenderness with a live fetus in breech presentation. Her total leukocyte count was 9200/c.mm. On ultrasonography, fluid in the peritoneal cavity mainly around uterus & Morrison pouch, few dilated bowel loops and live fetus were found. Clinical diagnosis of peritonitis was made on the basis of guarding, abdominal tenderness with clinical symptoms of vomitings and abdominal pain. Patient was kept nil orally on intravenous fluids. Ryle's tube was inserted and was kept on conservative management. Intravenous broad spectrum antibiotics were started. After two days of conservative management, she was taken up for emergency cesarean section in view of fetal distress. Intraoperatively, appendix was perforated and gangrenous (Figure 1) with diffuse pus flakes over the uterus, ovaries and gut loops. Appendectomy with peritoneal lavage was done. A live birth weighing 2.12kg with APGAR score of 7, 8 was executed. Postoperatively, she recovered well with no fetal or maternal morbidity. Histopathological examination of appendiceal specimen confirmed appendicitis.
Twenty five years old pregnant lady presented with complaints of generalized pain abdomen, more in the periumbilical area, constipation and fever for past four days at 30+6 weeks of period of gestation. She was hemodynamically stable, afebrile with no guarding or rigidity and carried a live fetus. On evaluation, her total leukocyte count was 10000/cmm, prothrombin index of 60%, and normal renal function tests. On ultrasonography, bilateral pleural effusion, dilated bowel loops with free fluid in the peritoneal cavity with air foci in it suggestive of pneumoperitoneum were found. Decision for laparotomy was taken in view of suspected bowel perforation. Exploratory laparotomy followed by appendectomy, peritoneal lavage and bagota bag application was done. Intraoperatively, there was 100ml of purulent fluid in peritoneal cavity, pus flakes were present in right paracolic gutter and appendix was inflamed and indurated with suspicion of sealed perforation. Rest of the bowel loops and other viscera appeared normal. Histopathology of appendicular specimen was suggestive of appendicitis. On second postoperative day, her urine output decreased. She developed respiratory distress for which she had to be put on assisted ventilation. Dialysis was initiated for maternal renal failure but intrauterine fetal death and maternal cardiac arrest occurred during dialysis and she could not be revived.
Acute abdomen in pregnancy is of serious concern to the obstetrician as lives of the both the mother and the fetus are at risk. The differential diagnosis include acute appendicitis, acute pancreatitis, acute cholecystitis, intestinal obstruction or perforation, hepatic rupture, ruptured ectopic pregnancy or ovarian cyst, adnexal torsion, degenerating fibroids, uterine rupture etc [2].
Acute appendicitis is the most common non obstetric surgical complication during pregnancy which can result in significant morbidity and mortality if not diagnosed and treated rapidly [1]. Physiological changes of pregnancy alter the clinical findings and laboratory values (total leucocyte count) used for diagnosis of appendicitis. The use of certain diagnostic procedures like X-ray abdomen is limited because of its teratogenicity [1].
The incidence of appendicitis (0.1%) during pregnancy is same as in non pregnant women without any predilection for any trimester of pregnancy [1,3]. The appendix lies in the right iliac fossa in the first trimester, reaching pelvic brim in the second trimester and right upper quadrant in the third trimester with resultant upper and more lateral pain in the abdomen as compared to non-pregnant [1]. Our both patients presented in third trimester with pain localization to epigastrium in first patient and periumbilical area in the second patient. It is difficult to elicit guarding and rigidity in third trimester due to consequent stretching of abdominal muscles [1]. The enlarged uterus lifts away the appendix from the abdominal wall leading to diminished irritation of parietal peritoneum [1]. The mean leukocyte count in patients with appendicitis had been found to be nearly same in patients with normal appendix indicating that leukocytosis itself, is not a clear predictor of appendicitis in pregnancy [3]. Detection rate of appendicitis by ultrasonography is very low ranging from 35–39% [1,4]. The specificity and sensitivity of ultrasonograhy alone was 99.2 and 12.5%, respectively [5]. The low sensitivity of ultrasonography is due to various reasons: operator dependency, obesity, obscuration by bowel gas and anatomic variations [6]. Wallace et al did a meta-analysis and analyzed the rates of negative appendectomy in three groups – one with clinical diagnosis only, second group diagnosed by clinical plus ultrasound and third group by clinical plus ultrasound plus CT scan and found rate of negative appendectomy as 54%, 36% and 8% respectively in three groups (p value <.05) [7]. But Computed tomography should be avoided during pregnancy because of risk of radiation exposure to the fetus [1]. MRI has been proven to be safe during pregnancy with high sensitivity for appendicitis (97% to 100%) [8].
Complications of pregnancy are more common following appendectomies in the first trimester and for perforated or gangrenous appendices [9]. Incidence of perforated diffuse peritonitis is high during pregnancy because infection is difficult to be confined to a localized area due to uterine contractions and omentum is unable to reach the inflamed appendix [1]. In a study by Mourad J. et al, rate of perforated appendix was higher during pregnancy as compared to non-pregnant cases (43 vs 15%) [3]. Risk of sepsis, pneumonia, postoperative infection, bowel obstruction and transfusion was higher in pregnant patients. This increased risk was mainly due to delay in diagnosis subsequent to upward displacement of appendix during pregnancy [10]. Both of our patients presented with appendiceal perforation and peritonitis.
The most encountered fetal complications reported by Andersen and Nielsen were spontaneous abortion (33%) and premature delivery occurred in 14% [9].
Treatment of appendicitis in pregnancy is primarily surgical. Early appendectomy should be performed whenever diagnosis of acute appendicitis is considered and is a key to success. Appendectomy should be performed as if pregnancy was not present. Site of incision is modified according to gestation towards right upper quadrant in the more advanced gestational age at the point of maximum tenderness. Surgery in unruptured appendicitis does not disturb the pregnancy [1]. Multidisciplinary team work by surgeon, obstetrician and anesthesiologist must be achieved to minimize maternal and fetal morbidity and mortality. A grossly normal appearing appendix should also be removed intraoperatively to avoid confusion of appendicitis in future for differential diagnosis of right lower quadrant pain [2]. A higher negative laparotomy rate (20-35%) in pregnancy is acceptable as compared to non pregnant patients (15%) due to difficulty in diagnosing acute appendicitis in a pregnant patient [1,11]. Delay in appendectomy increases the incidence of perforation to 66%, leading to grave consequences [1]. Laparoscopic appendectomy is safe, effective and valuable method for acute appendicitis in first or second trimester as it helps in easy localization of appendix with consequent right incision, thereby decreasing uterine manipulation and hence irritability [12]. However, with laparoscopic appendectomy, there is a rare chance of accidental injury to pregnant uterus with veress needle or trocar, effects of CO2 on pregnant patient and fetus and decreased uterine blood flow secondary to increased intra abdominal pressure resulting from pneumoperitoneum [13]. Wilasrusmee et al in a systematic review and metaanalysis compared the safety of laparoscopic vs. open appendectomy for appendicitis in pregnancy and found twofold increased risk of fetal loss with laparoscopic procedures [14]. Walker et al reviewed the literature and concluded that still there is insufficient evidence to suggest the preferred operative modality for acute appendicitis during pregnancy [15].
There is an insufficient evidence of conservative management of acute appendicitis in pregnancy as it increases the risk of maternal morbidity in the form of septic shock, peritonitis and venous thromboembolism. Risk of preterm labour has been estimated to be highest in non-operated group as compared to operated group [16].
Maternal mortality is nearly zero and is almost always associated with unconfirmed perforation and subsequent peritonitis as seen in our second case. In perforated appendicitis maternal mortality rate can reach up to 4% whereas fetal death can be as high as 43% [1,2]. Fetal mortality is high due to septicemia and prematurity [1], more in perforation.
To conclude, appendicitis in pregnancy has always been a challenge as compared to non pregnant women as it can topple the very existence of pregnancy itself by affecting both mother and the fetus adversely. It should always be considered in differential diagnosis of acute abdomen in pregnancy. The symptoms and signs of appendicitis in pregnancy are not different from that in a non pregnant except a slightly varied presentation in different trimesters of pregnancy. Early appendectomy is the treatment of choice at all gestations of pregnancy. Delay in surgery should not be afforded even at the cost of a negative laparotomy.

![]()

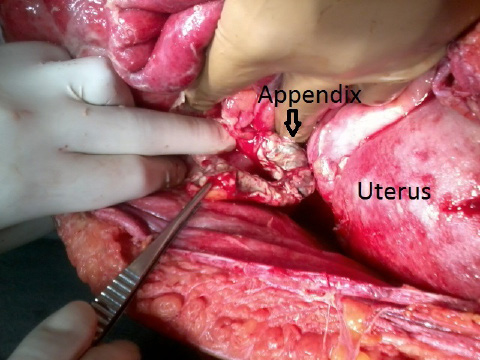 |
| Figure 1: Shows gangrenous appendix |




































