Open Access
Case Report
Max Screen >>
ISSN: 2455-7617
Copyright: © 2018 Binks M. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
A sizeable anastomotic leak post Ivor-Lewis oesophagectomy was managed by developing a right-sided thoracic oesophagostomy in a 66-year-old woman. At 18 months postoperatively, the patient is disease free and maintains a good quality of life.
Keywords: Thoracic Oesophagostomy; Ivor-Lewis Oesophagectomy; Anastomotic Leak
A 66-year-old woman with a cardioesophageal junction adenocarcinoma with proximal Barrett’s disease, was treated with Ivor-Lewis oesophagectomy in July, 2016. Despite neo-adjuvant chemo-radiotherapy and gastroscopic dilatation a month earlier, the tumour was completely obstructed and required feeding nasojejunal tube insertion a fortnight prior to surgery. She had previously undergone a right hemicolectomy for a caecal adenocarcinoma, a cone excision for cervical cancer and a right wide local excision with axillary node dissection for breast carcinoma.
The operation was complicated by extensive intra-abdominal adhesions and mesenteric tethering, which restricted the mobility of the gastric conduit. The proximal oesophagus was truncated by resection of a long segment of Barrett’s oesophagus. A colonic interposition was made impossible by the previous colonic surgery. The gastric conduit and oesophagus were anastomosed by hand with a single-layer of interrupted 3.0 PDS. The anastomosis appeared to be under no tension. An open feeding jejunostomy tube was placed and the patient had enteric feeds from day one.
A routine day three gastrograffin swallow showed no anastomotic leak. Histology revealed a poorly differentiated oesophageal adenocarcinoma (T2N0MX). On postoperative day nine, she was reviewed for fevers and rapid atrial fibrillation. She was septic with a C-Reactive Protein (CRP) of 387 and a loculated right-sided pleural effusion demonstrated on chest x-ray.
At relook thoracotomy, there were two large segments of anastomotic dehiscence with a right-sided empyema. The anastomosis was resected. To shorten operative time in a septic patient and retain the possibility of future reconstruction (jejunal graft conduit), the decision was made to create a right thoracic oeseophagostomy. A 28Fr intercostal catheter was sutured into the oesophageal stump and passed through the eighth intercostal space at the mid-axillary line and attached to a drainage bag. Jejunostomy feeding was continued indefinitely.
The patient was discharged following a period of rehabilitation. The intercostal catheter was removed after three months, with oral fluids passing freely into a stoma bag on the chest wall. The fistula tract has required dilatation on three occasions in the past 18 months. A 16Fr Foley catheter maintains patency and has prevented further narrowing.
At present, the patient tolerates oral fluids, is free of disease and enjoys what she describes as the best quality of life she has experienced in three years (Figure 1, 2 and 3).
Ivor-Lewis oesophagectomy uses a combined laparotomy and right thoracotomy to resect oesophageal and cardio-oesophageal cancer. The oesophagus is reconstructed by fashioning a neo-oesophagus out of the stomach, which is anastomosed to the remnant oesophagus in the chest. Between 20% and 80% of Ivor-Lewis oesophagectomies experience complications [1-4]. Patient age, premorbid physiological status, elective vs emergency surgery and department throughput all affect complication rates [5]. Respiratory complications such as atelectasis and pneumonia are the most common, whereas anastomotic leak is the most feared [4]. Others include systemic complications such as myocardial infarction and stroke and organ-space complications such as recurrent laryngeal nerve injury, chylothorax and bleeding [3].
Anastomotic leak complicates 0-35% of oesophagectomies and more than doubles both 30-day mortality and hospital stay [5-7]. The postoperative inflammatory milieu can make leak detection difficult and delayed, with diagnosis commonly at postoperative day 8 to 10 [8]. Screening contrast swallow studies and CT scans are of low sensitivity. Investigations such as CRP monitoring are emerging as a means of expediting leak detection [9-11].
Resuscitation, sepsis control and nutrition provision form the bedrock of managing anastomotic leakage anywhere in the gastrointestinal tract [7,12]. Definitive management of an oesophageal anastomotic leak is dependent upon duration since operation, symptomatology and patient stability [13]. Close surveillance, endoscopic therapies and open treatments are available to the treating surgeon. The latter is generally employed to manage early leaks with significant sepsis [7]. Sepsis control requires extensive lavage, decortication, debridement of necrotic and infected material and intercostal catheter insertion for ongoing drainage. When the dehiscence is limited, an attempt at primary closure of the defect is feasible [7,12,14]. If adequate conduit length is available, the anastomosis may be refashioned after resection of the diseased edges [7,14]. If this is impossible, or the leak is greater than two centimetres, near-circumferential or uncontained, oesophageal diversion by means of cervical esophagostomy may be life-saving [14]. Oesophageal diversion has proven an important salvage measure in other settings leading to mediastinitis, namely complicated hiatus hernias or their repair and iatrogenic or spontaneous oesophageal rupture [15]. The previous right hemicolectomy and extensive intra-abdominal adhesions present in the above case made future restoration of intestinal continuity fraught with difficulty if a cervical fistula was created. Although the patient is unlikely to opt for reconstructive oesophageal surgery in the near future, the decision to create a thoracic esophagostomy has retained the option.
To our knowledge, this is the first such case published in the literature with over 12-month follow up. The patient has received lifesaving and curative surgery, whilst maintaining a satisfactory quality of life. Whilst thoracic oesophagostomy confers a high degree of morbidity, it is important that general and upper gastrointestinal surgeons be aware of its potential to save life and the possibility of satisfactory postoperative recovery in certain settings such as that described.

![]()

 |
Figure 1: Lateral chest radiograph illustrating the 28Fr intercostal catheter placed in the distal oesophageal stump to promote fistula formation to the right postero-basal chest wall |
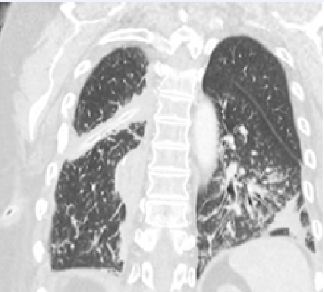 |
Figure 2: 12-month follow-up CT. The oesophagostomy has matured and traverses the posterior right hemithorax via the oblique pulmonary fissure |
 |
Figure 3: 12-month follow-up CT. The Foley catheter balloon can be seen in the proximal oesophageal stump |




































