Open Access
Research Article
Max Screen
ISSN: 2454-4981
Copyright: © 2021 Butt OH. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Diffuse midline gliomas with the histone 3-lysine-27-methionine (H3K27M) mutation should be considered in the differential diagnosis of recurrent hemiparesis and headache in patients with midline brainstem lesions, even with the absence of contrast-enhancement. Early diagnosis is essential for prognostication and engagement in trials evaluating novel therapeutics such as ONC-201.
Keywords: Primary Brain Tumor; Leptomeningeal Carcinomatosis; Diffuse Pontine Glioma; Stroke in Young Adults
List of abbreviations: CNS: Central Nervous System; CRP: C Reactive Protein; CSF: Cerebrospinal Fluid; GBM: Glioblastoma; H3K27M: Histone 3-Lysine-27-Methionine; HGG: High Grade Glioma; ICP: Intra-Cranial Pressure; IHC: Immunohistochemistry; MRI: Magnetic Resonance Imaging; WHO: World Health Organization
Recent advances in the molecular characterization of gliomas has radically changed our understanding of high grade gliomas (HGG), including glioblastomas (GBM). HGG represent a range of tumors which share glial features and poor overall survival, particularly for GBMs. In adults they are often lobar, with only 14% reported in deeper brain structures [1]. On magnetic resonance imaging (MRI), GBMs are traditionally associated with avid contrast enhancement with marked vasogenic edema. On pathology, GBMs are classically associated with diffuse, infiltrative, small, polymorphic cells with an increased nuclear to cytoplasmic ratio, high mitotic index, and with both highly vascularized and necrotic regions. However, the revised 2021 World Health Organization (WHO) criteria recognized several new categorizes of HGG which share the poor survival outcomes of traditional GBMs, while lacking either the traditional imaging or pathology features described above [2].
One such entity are midline gliomas carrying the histone 3-lysine-27-methionine (H3K27M) histone mutation [2-4]. H3K27M gliomas tend to occur in younger individuals with a particular pediatric/young adult bias for pontine lesions [5]. There is no gender predilection [3,6]. Ninety-three percent of pontine gliomas carry the H3K27M mutation [6]. Presenting symptoms vary based on location and extent of infiltration but commonly include cranial nerve palsies, hemiparesis, ataxia, nausea, vomiting, and headaches.
The propensity of H3K27M gliomas to mimic infectious or inflammatory lesions on imaging often results in delays in diagnosis with disastrous outcomes, as discussed in the following case. Early intervention is critical; with the experimental drug ONC-201 emerging as a promising therapeutic option. ONC-201 is a selective antagonist of the dopamine receptor D2/3 (DRD2/3) which targets the key pro-growth pathway in H3K27M gliomas.
A 21-year-old woman presented to an outside hospital with right arm and leg weakness, dysarthria, and drowsiness. Additional history revealed several weeks of new headaches, dizziness, nausea, and vomiting but no history of systemic or central nervous system (CNS) infections. Her exam was only notable for an unsteady gait. An extensive laboratory workup (Table 1) 27 nucleated cells/ µL (40% lymphocytes), protein of > 600 mg/dL, and no unique oligoclonal bands on cerebral spinal fluid (CSF) analysis. A CSF B. burgdorfi antibody was present (1.39 LIV, upper-limit of normal 0.99 LIV) but confirmatory western blot was negative. Aside from the aforementioned CSF studies, her laboratory workup was otherwise unrevealing. MRI of the brain demonstrated an isolated, non-enhancing, T2 hyperintense lesion in the pons (Figures 1A, B and C). She was treated with intravenous methylprednisolone and doxycycline for a presumed chronic CNS Lyme infection. Her symptoms completely resolved 5 days from onset and she was discharged home
She returned to the same facility two weeks later with left arm and leg weakness. A repeat brain MRI demonstrated an unchanged pontine lesion, despite earlier methylprednisolone and doxycycline (Figures 1D, E and F). A repeat Lyme IgG was again negative (Table 1). Concern for undertreated chronic Lyme disease prompted a 1-month course of doxycycline. Her symptoms again resolved in less than one week
Three months later, she was found down by her father and was obtunded on arrival to the outside hospital. Apnea during an MRI scan prompted urgent intubation. She received empiric dexamethasone and mannitol out of concern for elevated intra-cranial pressure (ICP) and she was transferred to our facility
Neurologic exam at our facility (off-sedation) showed her to be obtunded with a fixed 7 mm pupil OD and 6 mm minimally reactive pupil OS, absent corneal reflexes OU, a weak cough, and stimulus induced triple flexion in both lower limbs. Brain MRI (Figures 1G,H,I,J,K and L) revealed extensive bilateral cortical diffusion restriction concerning for infarction due to insufficient cerebral perfusion. The pontine lesion without contrast enhancement was minimally changed relative to prior. She underwent an extensive laboratory workup (Table 1). Notable abnormal findings included an opening pressure on lumbar puncture of > 55 cm H20. Cerebrospinal fluid analysis showed 102 nucleated cells/µL (77% neutrophils) and a markedly elevated protein of 488 mg/dL. Her C reactive protein (CRP) was also elevated (7.4 mg/L on arrival) but the remainder of her workup was unrevealing. No serum markers for ischemic injury were obtained
From her initial presentation, post-contrast T1 reveals a non-enhancing pontine hypointensity (A), with notable fluid-attenuated inversion recovery (FLAIR) hyperintensity observed in axial (B) and sagittal views (C). Minimal change is observed in postcontrast T1 (D), or FLAIR (E, F) imaging two weeks later. Approximately 3 months later, her pontine lesion is minimally enlarged on post-contrast T1 (G) or FLAIR (H). No susceptibility artifact is noted on blood sequences (I). Marked cortical edema is also appreciated on FLAIR (J), with striking diffusion restriction (K, M)
WBC = white blood cell; RBC = red blood cell; HSV = Herpes simplex virus; PCR = polymerase chain reaction; VZV = Varicella zoster virus; HHV = Human herpesvirus 6; Ab = antibody; FTA = fluorescent treponemal antibody; Ag = antigen; AFB = Acid fast bacillus; ANNA = Antineuronal nuclear antibody; AIME = Autoimmune encephalitis; HIV = Human immunodeficiency virus; ESR = Erythrocyte sedimentation rate; CRP = C-reactive protein; ANA = antinuclear antibody; ENA = Extractable nuclear antigen; ANCA = Antinuclear cytoplasmic antibody; dsDNA = Double-stranded DNA; ACE = Angiotensin converting enzyme; TSH = Thyroid stimulating hormone; RMSF = Rocky Mountain Spotted Fever; TPO = Thyroperoxidase. a PCR assay for: E. coli K1, H. influenzae, L. monocytogenes, N. meningitidis, S. agalacticae, S. pneumoniae, Cytomegalovirus, Enterovirus, Herpes simplex 1/2, Human herpesvirus 6, Parechovirus, Varicella zoster, Cryptococcus neoformans/gattii b Paraneoplastic autoantibody evaluation panel, Mayo Clinic, Rochester MN
Over the next 36 hours, the patient developed severe hypertension before becoming acutely hypotensive. Repeat head CT revealed worsening cerebral edema and multifocal hemorrhages, which soon thereafter progressed to diffuse cerebral edema despite external ventricular drain placement and aggressive medical management. Subsequent neurologic examination and apnea testing were consistent with brain death, likely due to diffuse cortical infarction from insufficient cerebral perfusion pressure in the setting of elevated ICP.
Autopsy showed a pontine glioma carrying the H3K27M mutation with diffuse cortical and leptomeningeal infiltration (Figure 2) Gross pathology revealed gyral effacement and patchy leptomeningeal opacification of the cerebrum (e.g. left Sylvian fissure) (Figure 2A), an ill-defined, expansile pontine lesion (Figure 2B), and hemorrhagic plaque-like lesions over the lumbosacral spinal cord (Figure 2C). Hematoxylin and eosin stained sections demonstrated an infiltrative glial neoplasm in the pons (Figure 2D). Immunohistochemistry (IHC) using a monoclonal antibody directed at the abnormal H3K27M protein was diffusely positive (Figure 2E), with drop metastases noted in the throughout the cord (Figure 2F and G).
Lateral view of the left cerebral hemisphere (A) demonstrating gyral effacement due to cerebral edema, with hazy opacification of the leptomeninges surrounding the Sylvian fissure. Cross sections of the pons (B) reveals an ill-defined, expansile rightsided lesion obfuscating the transverse pontine fibers. The lumbosacral spinal cord (C) features hemorrhage and tan plaquelike lesions in the subarachnoid space. Hematoxylin and eosin stained (H&E) sections of the pontine lesion (D, original magnification x 400) demonstrate marked hypercellularity of a diffusely infiltrating glioma (note the entrapped neuron within the pontine parenchyma). IHC for H3K27M (E, original magnification x 400) shows strong and diffuse reactivity in tumor cell nuclei and nonreactivity in background non-neoplastic cells. H&E section of the plaque-like lesions in the cervical cord show drop metastases in the subarachnoid space (F, original magnification x 200). These discrete tumor nodules in the subarachnoid space were also patchily present in the cerebellum and cerebrum, corresponding to areas with hazy leptomeninges. In the lumbosacral cord, fibrinous exudate and hemorrhage are seen accompanying the tumor cells (G, original magnification x 400)
Midline gliomas carrying the H3K27M mutation represent a unique subgroup of gliomas. They often mirror high-grade gliomas with poor prognosis, despite at times lacking classical histologic features and/or lacking classical imaging features [2-4]. Leptomeningeal spread has been documented in approximately 1/3 of cases [7]. Early fulminant spread is rare, with only a single case of fulminant spread of an H3K27M mutant glioma previously reported in adults [8,9]. In this case, fulminant leptomeningeal infiltration resulted in progressive increase in ICP and eventual loss of cerebral perfusion. Early fulminant leptomeningeal spread of an aggressive neoplasm should remain on the differential for idiopathic diffuse ischemic injury with a focal pontine lesion
Early diagnosis is critical for all HGG, including H3K27M mutant gliomas. Coordination with neurosurgery to obtain a tissue sample is strongly encouraged. This is particularly true after an extensive inflammatory and infectious workup is otherwise unrevealing, as in this case. Tissue may be acquired from biopsy or tumor debulking. Unfortunately, given their common locations, these tumors are often not amenable to surgical debulking. When biopsy is not an option, close clinical follow up with serial imaging and referral to neuro-oncology specialist is critical. Progressive symptoms in the setting of a suspicious lesion not amenable to biopsy may warrant empiric treatment. Early intervention in this case may have delayed leptomeningeal spread and provided a meaningful prolongation of survival.
Standard treatment mirrors that of other HGG (i.e. a 6 week course of high-dose fractionated radiotherapy (60Gy) and concurrent temozolomide, followed by 6 cycles of monthly adjuvant temozolomide) with mixed results. Promising Phase 1 results from the ONC-201 clinical trial (NCT02525692) offers hope for a new class of targeted therapies [10,11]. Notably, leptomenginal spread was excluded as part of NCT02525692, with its efficacy in similar cases as presented here remaining unknown. Nonetheless, promising preliminary results of the phase II studies involving ONC-201 highlight the importance of referral to specialty centers and consideration for the expanded access trial, study ONC-028 (NCT04617002).
We would like to give special thanks to the family of the patient

![]()

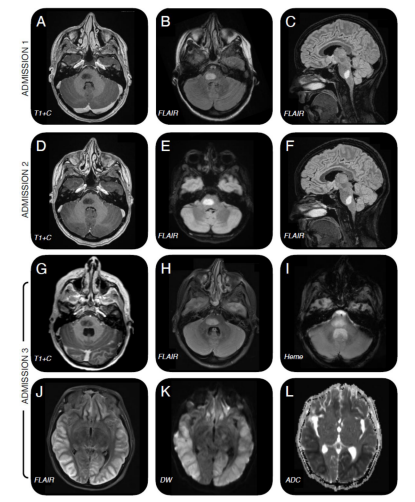 |
| Figure 1: MRI Findings during three admissions |
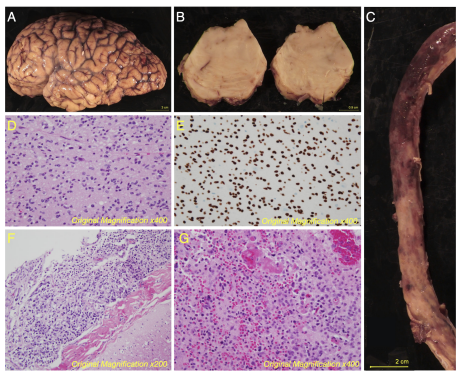 |
| Figure 2: Histopathological findings at Autopsy |
CSF Studies |
Admission 1 |
Admission 2 |
Admission 3 |
Admission 3 |
WBCs |
27 |
|
59 |
102 |
% neutrophils |
34 |
|
8 |
77 |
% lymphocytes |
50 |
|
66 |
2 |
% monocytes |
16 |
|
26 |
21 |
RBCs |
111 |
|
541 |
10490 |
Glucose |
52 |
|
43 |
100 |
Protein |
>600 |
|
469 |
488 |
IgG Index |
0.64 |
|
0.45 |
|
Albumin Index |
194.2 |
|
112 |
|
Oligoclonal bands |
0 |
|
0 |
|
Meningitis panela |
negative |
|
negative |
|
HSV PCR |
negative |
|
negative |
negative |
VZV PCR |
|
|
|
negative |
Enterovirus PCR |
negative |
|
negative |
negative |
HHV-6 PCR |
|
|
|
negative |
Toxoplasma PCR, IgM, IgG |
|
|
|
negative |
B. burgdorferi Ab |
1.39 |
|
0.41 |
|
FTA |
negative |
|
negative |
|
West Nile IgM/IgG |
negative |
|
negative |
negative |
Cryptococcus Ag |
negative |
|
negative |
negative |
Bacterial culture |
no growth |
|
no growth |
no growth |
Fungal culture |
no growth |
|
|
no growth |
AFB culture |
no growth |
|
|
|
Cytology |
no malignancy |
|
no malignancy |
|
ANNA Ab |
|
|
negative |
|
Serum Studies |
|
|||
AIMEb |
|
|
|
negative |
HIV |
|
|
negative |
negative |
Syphilis Ab |
|
|
negative |
negative |
Lyme IgG |
negative |
negative |
|
negative |
ESR |
|
|
30 |
16 |
CRP |
|
|
7.4 |
16.2 |
ANA |
negative |
|
negative |
negative |
ENA |
|
|
|
negative |
ANCA |
|
|
negative |
negative |
Rheumatoid Factor |
<10 |
|
12.2 |
<10 |
dsDNA |
|
|
negative |
|
Anticardiolipin |
negative |
|
|
|
C3 |
96 |
|
|
79 |
C4 |
16 |
|
|
13.4 |
ACE |
26 |
|
11 |
|
Procalcitonin |
|
|
0.03 |
|
TSH |
|
|
1.81 |
0.49 |
Ehrlichia IgG/IgM |
|
negative |
|
|
RMSF IgG/IgM |
|
negative |
|
|
Vitamin B1 |
|
|
|
112 |
TPO Ab |
|
|
|
<20 |
Tocopherol |
|
|
|
5.6 |
Vitamin A |
|
|
|
16.6 |
VZV IgG |
|
|
|
positive |
Hepatitis panel |
|
|
|
negative |




































