Open Access
Research Article
Max Screen >>
ISSN: 2454-4981
Copyright: © 2017 Pontes CM. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Marchiafava-Bignami disease (MBD) is a neurological disorder that has been found to be associated with chronic alcoholism and malnutrition. We report a 45 year old man, chronic alcoholic that developed discouragement for activities involving daily living, changes in retrograde memory in addition to mutism and gait instability. Brain MRI showed central atrophy of the corpus callosum(CC), hypointensity(necrosis) and ventricular dilation(white matter and subcortical region involvement). Pathological characteristics include isolated demyelination and axonal loss in the central layer of the CC sparing the dorsal and ventral layer. This pattern of necrosis of the middle layer of the CCis a typical finding in the disease. The clinical diagnosis has considerably changed during recent decades after brain MRI provided the opportunity of a reliable in-vivo diagnosis. With early detection and treatment, the prognosis of MBD may be good.
Keywords: Marchiafava-Bignami disease; Corpus callosum; Cronic alcoholic
Marchiafava-Bignami disease (MBD) is a rare complication related to alcohol abuse and chronic malnutrition which results in demyelination and symmetrical necrosis of the central layer of the corpus callosum [1]. Serum anion gap and osmotic gap can be observed in patients ingesting etanol. The serum anion gap still might be high, which could lead to the demyelination syndrome. The increase in serum osmolarity produced by alcohol is relied onserum concentration, molecular weights, and metabolic rate. Toxic effects of alcohol and its metabolites can cause demyelination of the corpus callosum [2]. Despite alcohol is the principal element, there are other causes that can be factors such as cyanide and CO poisoning, sepsis, sickle cell disease and Plasmodium infection [3]. The clinical presentation is variable, including mental confusion, dementia, psychosis, spasticity and dysarthria [4]. Since the symptoms are not specific, the clinical diagnosis can be difficult, being the magnetic resonance imaging (MRI) of pivotal value in the investigation [5]. Diffuse thickening of the CC andT1 and T2 prolonged areas in the CC are considered characteristic MRI findings at the acute phase. It has been reported that the first change on MRI is diffuse swelling of the corpus callosum, followed by a genu lesion, and finally by a splenium lesion, sparing the rostrum [5,6]. T1-weighted MRI in the subacute to chronic stage shows hypointense cystic-necrotic lesions in the corpus callosum in addition to callosal atrophy. Extracallosal lesions have been reported involving predominantly the periventricular white matter or the basal ganglia [7].
Man, 45 years old, bus driver and chronic alcoholic. According to his wife’s report, in April 2014 he developed changes in executive skills, inattention, gait instability and alteration in memory for spatial layouts(ability to recognize environments learned long time ago). Progressive worsening occurred with dysarthria which resulted in mutism after 6 months. On examination there was gait instability. During hospitalization he performed blood tests such as VDRL, TPHA, anti-HIV 1 and 2, anti-HTLV 1 and 2, hepatitis B and C, vitamin B12, all with values normal. Magnetic resonance imaging of the skull demonstrated atrophy of central portion of the corpus callosum and focus of hypointensity compatible with necrosis, in addition to ventricular dilation. The patient was treated with vitamin B1 (300 mg/day) and vitamin B12 (5000 mcg/day) resulting in a great improvement in mutism, gait instability and inattention. There had been partial resolution of radiological signs after six months Figure 1a,1b,1c and 1d.
MDB was described in 1903 by two Italian neuropathologists, Ettore Machiafava and Amico Bignami who observed three chronic alcoholics with symptoms of psychomotor agitation, convulsions, and declining level of consciousness [1,8]. All patients died after having seizures and coma. In each one, the middle two thirds of the corpus callosum was found to be severely necrotic. Neuropathological studies have revealed demyelination and corpus callosum atrophy [9]. Until recently, the definitive diagnosis of MBD could only be confirmed at necropsy. However, with the advent of neuroimaging, it was possible to define it through the previous history of alcoholism and pathological changes in the corpus callosum, demonstrated by means of MRI [10]. On the past (1977) Brion et al had introduced a classification for MBD categorizing an acute, a subacute, and a chronic form [5].
• Acute state - seizures, alterations of consciousness, and death may occur.
• Subacute state - characterized by mental confusion,behavioral disorders, memory deficits, cerebellar signs and interhemispheric disconnection.
• Chronic state - mild dementia.
Whereas the above mentioned clinical classification is still widely used, Heinrich et al proposed a clinicoradiologic classification considering the patients’s clinical status as well as the radiological severity of cerebral changes detectable in MRI. In 2004 they stressed, that the terms “acute,subacute and chronic” should be abandoned to describe a subtype of MBD. Cases can be assigned to one of two groups, which they refer to as type A or type B, based on a review of 50 radiologic cases diagnosed in vivo:
Type A- Predominant features of coma and stupor, seizures, limb hypertonia; this subtype is associated with a high prevalence of pyramidal tract symptoms. Radiologic features include involvement of the entire corpus callosum.
Type B - Normal or mildly impaired mental status, rapid onset of dementia, limb hypertonia, dysarthria and astasia-abasia. It was considered typical for subacute forms. Radiologic features are partial or focal callosal lesions. Type B has favourable prognosis and lesions may reverse suggesting an underlying edema rather than demyelination [7].
At present, the diagnosis is made on the basis of clinical findings in combination with radiological imaging features [11] Table 1.
The corpus callosum is the largest commissural white matter bundle in the brain containing 200-250 million interhemispheric fibers [12,13]. Major portion of the corpus callosum receives its arterial supply from the carotid system except for splenium, which is supplied by the vertebrobasilar system [14]. MRI is currently the most sensitive diagnostic tool as well as to monitor the evolution toward partial or total regression [11,15]. Acute or subacute lesions are characterized by edema and early myelin damage. The corpus callosum lesions are hypo-intense on T1-weighted image and hyperintense on T2-weighted/fluid-attenuated inversion recovery (FLAIR) images. Fast spin-echo and T2-weighted MRI scans show hyperintensity with nonenhancing on postgadolinium images [8]. During the subacute phase, cystic lesions begin to develop. In chronic stage hypointensity on T1-weighted images is mainly related to a total loss of myelin, with necrosis, gliosis and replacement of the region by a cyst and residual atrophy of the involved structures [15]. FLAIR images may show central hypointense signal and peripheral hyperintense rim (“Sandwich sign”) [8]. Another signal that can be observed is hiperintensity involving the entire splenium (“Boomerang sign”) [12]. Although the callosal lesions have been described as the hallmark of this disease, few cases of MBD also demonstrate signal intensity abnormalities in frontal lateral and temporal cortices (Morel’s cortical laminar sclerosis) [16]. Other imaging modalities include MR spectroscopy (MRS) which shows increase in choline and increased choline/creatine (Cho/ Cr) ratio in acute phase. Lactate peak is usually seen in the acute/subacute phase of demyelination. SPECT studies show bilateral cortical and/or subcortical hypoperfusion. This perfusion defected notes that the disease doesn’t only affect corpus callosum [12,17,18]. The aim of serial MR imaging and MR spectroscopy in Marchiafava-Bignami disease is to note changes after vitamin therapy and to assess the contribution to in vivo study of the disease[16].
Differential diagnosis includes infarction of recurrent artery of Heubner , neoplastic disease such as astrocytoma or lymphoma of corpus callosus, demyelinating disease such as multiple sclerosis (MS), Wernicke encephalopathy, progressive multifocal leukoencephalopathy, HIV related encephalopathy, neurosyphilis and acute disseminated encephalomyelitis [19].
Strict alcohol abstinence with counseling is the best core of the treatment program. Pharmacological treatment consists of administration of thiamine IV 500 mg three times a day (TID) for 3 days and then 100 mg per os (PO) [20]. Also clinical improvement could be observed using high dose of corticosteroids(250 mg methyl-prednisolone ), others B-complex vitamins, folic acid and amantadine (100mg 2x per day) [21-23]. The available evidence suggests that an effective and aggressive early treatment is often associated with marked clinical improvement [24].
Advances in neuroimaging have made early diagnosis of MBD possible and help in early initiation of treatment. Clinical evidences support that clinical improvement of patients with MBD is associated with radiological improvement as well. Fast and near-complete relieve of symptoms is possible, even though involvement of the entire corpus callosum and the cortex. MBD may be a reversible brain disease.

![]()

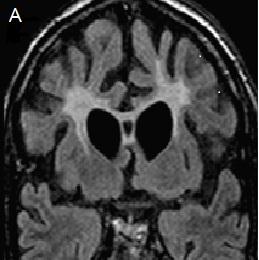 |
| Figure 1a: Coronal flair showing demyelination of corpus callosum and commitment of periventricular white matter Sagital |
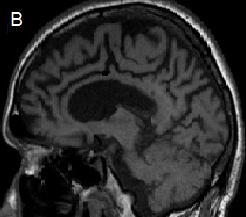 |
| Figure 1b: Sagital T1 showing necrosis in splenium of corpus callosum |
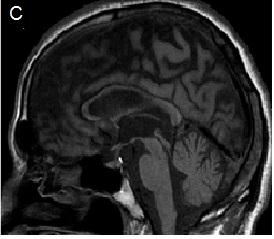 |
| Figure 1c: Sagital T1 showing diffuse tapering of corpus callosum("Sandwich sign") |
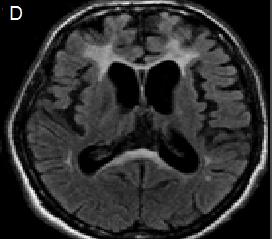 |
| Figure 1d: Axial flair showing periventricularcommitment of genu and splenium("Boomerang sign") in addition to cerebral atrophy |
MRI findings |
Underlying pathophysiology |
|---|---|
Hyperintensity on T2 weighted images |
Edema and myelin damage |
Hypointensity on T1 weighted images |
Total loss of myelin with replacement of the region by a cyst |
Hyperintense rims and hypointense cores on FLAIR images |
Damage to the myelin at the rim with a central necrotic area |
Uniformly hyperintense lesions on FLAIR |
Mixture of demyelination and edema |
Areas of restricted diffusion on DWI (acute phase) |
Cytotoxic edema |
| Table 1: Correlation of imaging findings in MBD with pathophysiology | |




































