Open Access
Research Article
Max Screen >>
ISSN: 2393-9060
Copyright: © 2016 Arani KS. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background & Objective: Both high prevalence of poor vitamin D status and obesity in children and adolescents are known health problems, but there is not enough information about adequate dose of vitamin D to treat these children. The aim of this study is to evaluate the efficacy of an oral vitamin D regimen for this problem.
Material and Method: In this clinical trial 100 children and adolescents with vitamin D deficiency or insufficiency were participated. The vitamin D deficiency defined as 25OHD ≤ 15 ng/ml and vitamin D insufficiency as 15 ≤ 25OHD ≤ 20 ng/ml. In terms of obesity, individuals were classified in two groups: obese & overweight (57 subjects) and normal weight (43 subjects). All subjects received 50000 IU vitamin D once a week for 6 weeks, and the 25OHD level was measured 2-6 months later.
Result: The mean 25OHD level before treatment in first group (obese & overweight) was 10.74±5.96 ng/ml and in normal weight group was 10.81±5.41 ng/ml. (P=0.54) Average levels of 25OHD after initial treatment was 33.64±22.43 ng/ml and 37.66±17.74 ng/ml respectively (P=0.6) The frequency of vitamin D deficiency and insufficiency after initial treatment was 12.8% and 9.3% respectively.
Conclusions: This study showed that treatment with 50000 IU Vitamin D weekly for 6 week is a safe and effective regimen for majority of Vitamin D deficient or insufficient children regardless of obesity status.
Keywords: Vitamin D deficiency; Vitamin D insufficiency; Obesity; Children
Vitamin D deficiency is a common health problem over the entire world and recognized as a pandemic [1,2]. Foods naturally contain very small amount of vitamin D, and fortified foods with vitamin D are often inadequate to satisfy vitamin D requirements [2]. So the major cause of vitamin D deficiency is the inadequate sun exposure. In the recent years many reports have been published about the high prevalence of vitamin D deficiency in obese children and adolescents, also obesity epidemic between teens is rising [3-6]. A prospective study showed that serum 25 hydroxy-vitamin D (25OHD) level is inversely associated with the development of adiposity in children [7]. Severe vitamin D deficiency leads to myopathy, clinical rickets in children, and osteomalacia in adults [8,9]. In addition to musculoskeletal effects, vitamin D is also important for immune system performance , and vitamin D deficiency is probably linked with a variety of diseases including: hypertension, cancer, diabetes and multiple sclerosis [8,10,11]. The prevalence of vitamin D deficiency varies from 44.8% to 79.6% in Iran [12-14]. The vitamin D level lower than 20 ng/ml is associated with decrease in the function of pancreatic cells and lower insulin sensitivity [15]. The correction of vitamin D level can increase the insulin sensitivity in obese children [16,17]. The serum 25OHD levels to a lesser extent or equal to 15 ng/ml has been suggested as the threshold for negative effects of vitamin D deficiency on the level of insulin sensitivity in obese African American girls [18]. The study of Weaver, et al. (2004) has shown that the 32 ng/ml serum level of 25OHD is required for the proper absorption of calcium and adequacy of the parathyroid hormone suppression [19]. However, there are insufficient data about the ideal vitamin D regimen to correct 25OHD level in healthy children and adolescents. Multiple therapeutic regimes have been introduced for this problem, each one has benefits and restrictions. Some of these vitamin D regimens are as follows: 50,000 IU weekly for 6-8 weeks [20], 50,000 IU weekly for 4 weeks then monthly for 5 months, 50,000 IU three times a week for 6 weeks [21], two doses of 100,000 IU vitamin D with the three-month interval [22]. The aim of this study is to evaluate the effect of an oral vitamin D regimen for treatment of vitamin D deficiency in obese children and adolescents.
This study was conducted as a before-after clinical trial on the obese and overweight children and adolescents with vitamin D deficiency or insufficiency between 2 to 18years old from june 2013 until November 2014. The study design was approved by ethical committee of Kashan University of Medical Sciences and written consent was obtained from the parents of patients. All participants were examined by a pediatric endocrinologist. Exclusion criteria included the following: 1) recent use of vitamin D preparations (for last six months), 2) the disorders of the calcium, phosphorus and vitamin D metabolism, 3) the use of medication affecting vitamin D metabolism such as antiepileptics and estrogens, 4) malabsorbtion disorders such as celiac disease, cystic fibrosis, etc. 5) endocrine disorders such as cushing’s disease, hypothyroidism, pseudohypoparathyroidism, etc. 6) any acute or chronic illness, 7) the use of alcohol or tobacco.
The weight, height, body mass index (BMI) and pubertal stage were determined. BMI was calculated as weight (kg) divided by height2 (m). The subjects were divided upon BMI using the CDC (Centers for Disease Control and Prevention) growth charts to three groups: 1) Obese: BMI at or above the 95th percentile for age and gender, 2) Overweight: BMI at or above the 85th percentile and lower than 95th percentile for age and gender, 3) Normal weight: BMI lower than 85th percentile for age and gender [23]. BMI-SDS were calculated on the basis of 2000 normative data from the CDC.
Serum level of 25OHD level was measured using the chemiluminescence assay (DiaSorin, LIAISON® 25 OH Vitamin D assay). Vitamin D deficiency was defined as a serum 25OHD level of < 15 ng/ml and vitamin D insufficiency as a 25OHD level of 15–20 ng/ml [24,25]. Vitamin D sufficiency have been considered as serum 25OHD concentrations of 20 ng/ml or greater [24]. Subjects with vitamin D deficiency or insufficiency were treated with one pearl of vitamin D (50,000 IU) once a week for 6 weeks. Vitamin D3 pearls were provided by Alhavi Company Iran. A second blood sample for the measurement of 25OHD level was obtained 2-6 months later. This trial was registered in Iranian Registry of Clinical Trials (IRCT), No. IRCT2014090812421N2.
Statistical analysis was performed using SPSS, version 16.0 (SPSS software Inc, Chicago, IL, USA). Values of descriptive data were presented as mean±standard deviation. P values lesser than 0.05(two-sided) were considered statistically significant. No imputations of missing data were made. Baseline characteristics of participants were compared using either independent t tests (continuous) or chi-square tests (categorical). After treatment, changes between-group from baseline were analyzed repeated-measures ANOVA.
From 328 children and adolescent with vitamin D deficiency or insufficiency who treated with vitamin D only 141 subjects came for second sampling (45 obese, 29 overweight, 67 normal weight). Some patients due to the difficulty in taking the pills, were treated by vitamin D injection, so they were excluded. Finally 101 children remain in the study (34 obese, 23 overweight and 43 normal weight). The mean age was 10.04±3 years and the mean BMI was 21.18±3.96. The subjects were classified into two groups: 1- obese and overweight (57 individuals) 2- normal weight (43 individuals). Two group have not significant difference in time of sampling (P=0.86). The average level of serum 25OHD was 10.74±5. 96 ng/ml and 10.81±5.41 ng/ml respectively (P=0.54). The average level of 25(OH)D was 33.64±22.43 ng/ml and 37.66±17.74 ng/ml respectively after the first course of treatment (P=0.6). A significant difference was observed between the 25OHD level before and after treatment (P=0.02) (Table 1). Both sex had similar response to treatment (P=0.45).
The mean difference between the serum 25OHD level before and after treatment, was 26.28±18.54 in normal weight and 24.13±22.14 ng/ml in Obese & overweight group respectively (P=0.355).
The mean difference between the serum 25OHD level was 25.87±20.3 before and after treatment, however the relationship was not significant within weight groups (P=0.365) and sex (P=0.394). After initial treatment, the frequency of vitamin D deficiency and insufficiency was 12.8% and 9.3% respectively, and 77.9% had serum 25OHD level over than 20 ng/ml.
To evaluate the duration of effect of this regimen, second measurement of serum 25OHD was done 2-6 months later. In those subjects that sampling was done before 75 days from treatment onset (mean 60 days), the mean serum 25OHD was 41.03±20.94 ng/ml and in group with sampling after 75th day (mean 128 days) was 28.19±13.15 ng/ml. (P < 0.0001). The mean difference between second and first serum 25OHD level was 29.77±21.29 before 75th day and 19.55±12.89 after 75th day (P=0.007) (Figure 1)
Different definitions of vitamin D deficiency and insufficiency have been used in researches. Vitamin D deficiency was defined as serum 25OHD less than 15 ng/mL [24,26], less than 10 ng/mL [5,27] and less than 20 ng/mL [5,21,28]. There is insufficient data about ideal regimen for treatment of vitamin D deficiency in children. Also there is controversy about response to treatment in obese children in comparison with other children. This study showed that obese children have similar response to treatment in comparison with normal weight children. We used the total dose of 300,000 units Vitamin D using 50000 IU Pearls weekly for 6 doses. This treatment causes the elimination of vitamin D deficiency or insufficiency in 77.9% of subjects (25OHD > 20 ng/mL) and 53.9% of them achieved serum 25OHD over 30 ng/mL. Our treatment method was similar to regimen that used by Harel, et al. (2011). They treated 43 vitamin D deficient obese children (25OHD less than 20 ng/mL) aged 1-17 years with 50,000 IU of vitamin D once a week for 6-8 weeks, but only 28% of subjects achieved serum 25OHD over 30 ng/mL [20].
Another study that had similar results to our study has been performed by Malabanan, et al. They used 50,000 IU vitamin D once a week for 8 weeks and 60% of subjects achieved serum 25OHD over 30 ng/ml [29]. We did not find a significant difference between overweight or obese children with normal weight children in response to the above regimen but Rajakumar, et al. reported that obese children have less response to the treatment in 41 African –Americans children [et al]. In a study in Argentina, 15 healthy 10-18 years old teens with vitamin D deficiency, received two doses of 100,000 units of vitamin D with the three-month interval since the start of the winter, after the second dose, the 25OHD in all subjects reached to more than 15 ng/ml and none of the children had not 25OHD levels over than 50 ng/ml [31]. In a clinical trial in Yazd (Iran) 120 vitamin D deficient middle school aged girls received four different therapeutic regimen, those regimens starting with 300,000 units vitamin D and continuing with 50000 units monthly or 1000000 units each three month have the best results [22].
In a medical center in Atlanta , Pepper, et al. evaluated three different regimens for vitamin D deficiency for 306 adult patients: 1) 50,000 units vitamin D once a week for four weeks and then monthly until 6 months. 2) 50,000 units vitamin D once a month for 3-6 months, 3) 50,000 units vitamin D three times a week for a period of 6 weeks. All three regimen increased 25OHD level but optimal levels of 25OHD (> 30 ng/mL) achieved respectively 38%, 42% and 82% [21].
One of the important points in the treatment of vitamin D deficiency is sustainability of a treatment regimen. Our study has shown that serum 25OHD level had a drop after two months gradually, Harel, et al. also showed similar results [20] and this is against the injection of single-dose of 300,000 unit vitamin D that serum 25OHD level has a more gradual increase. Hashemipour, et al. (2005) was shown that serum 25OHD level after injection of single-dose of 300,000 unit vitamin D is increasing up to 4 months [32]. The level of serum 25OHD three months after intramuscular administration of 300000 units vitamin D was higher than previous determinations and was associated with increased serum levels of FGF-23 that accompanied by increasing the bone absorption [33].
Diamond, et al. showed that the effect of intramascular injection of 600000 IU vitamin D to vitamin D deficient patients persist up to 12months after treatment [34].
This study showed that the 50000 IU vitamin D weakly for six dose is a safe and effective regimen for treatment of vitamin D deficiency or insufficiency in children and adolescents.
According to the results achieved in this study, we recommend to study the impact of 50000 IU vitamin D weakly for 8 weeks and then monthly for 6 months for treatment and prevention of recurrence of vitamin D deficiency or insufficiency in children and adolescents.

![]()

Weight groups |
Sex |
25OHD
(pretreatment) |
25OHD
(posttreatment) |
P value |
||
N |
mean ±SD |
N |
mean ±SD |
p=0.02 |
||
Obese &overweight |
Male |
12 |
5.04 ± 11.31 |
12 |
29.24 ± 38.69 |
|
Female |
26 |
5.25 ± 9.32 |
26 |
22.47 ± 30.33 |
||
Normal weight |
Male |
12 |
3.66 ± 11.85 |
12 |
13.6 ± 36.45 |
|
female |
26 |
6.31 ± 10.31 |
26 |
19.98 ± 39.8 |
||
| Table 1: Comparison of the serum 25OHD before and after treatment in terms of weight groups and sex | ||||||
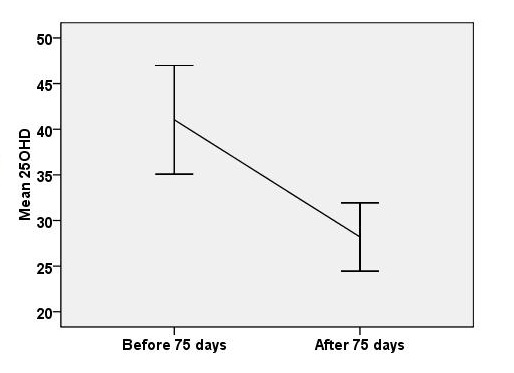 |
| Figure 1: Comparison of 25OHD after treatment in terms of time |




































