Open Access
Research Article
Max Screen >>
ISSN: 2394-6512
Copyright: © 2021 Ariff S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Introduction: Infectious meningitis is caused by infectious agents such as bacteria, viruses, fungi, and other agents. The viruses can cause a higher incidence of meningitis than that of bacteria and other infectious agents but the infection is usually less severe than others. Among the viruses, enteroviruses are reported to be the most common particularly in the developed countries.
Case Description and Conclusion: A teenager aged 17 years was taken to the Accident and Emergency with clinical signs of headache, sensitive eyes to light, fever, and neck stiffness. After diagnosis, he found to have meningitis so that he started directly with antibiotic treatment and blood samples are collected for biochemistry tests, bacterial culture, CT ( or MRI) scan as well as for antibody testing and mumps PCR because her sister has been diagnosed as having mumps. However, all tests were found negative or normal. On the second day, the patient's health became worsen and He has also become drowsy and lethargic; therefore, he was advised to start with an antiviral (acyclovir) and samples taken for viral diagnosis by PCR and the result was found enterovirus positive.
Keywords:Enterovirus Meningitis; Aseptic Meningitis; Viral Meningitis; Infectious Meningitis
Meningitis is inflammation of the meninges and cerebrospinal fluid (CSF) and it is usually characterized by headache, fever, stiff neck, and photophobia. It is caused by many infectious and non-infectious agents but viruses are now more common and the disease is known as viral (aseptic) meningitis. Among the viruses, enteroviruses are common to cause meningitis, especially in developed countries. The disease is usually self-limited and may recover completely within 7 to 10 days [1-3]. However, some enteroviruses can rarely be more severe and may progress to meningoencephalitis or encephalitis that are considered fatal or may associate with significant morbidity. Therefore, it is important to diagnose the disease as early as possible and detection of the virus in the CSF of the infected patients, which is now possible by PCR (Real Time-PCR), to apply the early treatment. However, the specific antiviral agent is not available against enteroviruses yet; the number of hospital admission and the mortality rate may be reduced by a restricted preventative and control measure [1].
A teenager aged 17 years was taken by his parents to the Accident and Emergency (A & E) because he has developed a headache and complained that bright light hurts his eyes. When examined in A & E, it is found that he has fever and neck stiffness as well. He was diagnosed to have meningitis so that the doctor has given him 1 gram of antibiotic ceftriaxone. For further diagnosis, blood samples are collected for biochemistry tests, a whole blood count, and bacterial culture. Cerebrospinal fluid (CSF) is also collected using the lumbar puncture technique. It is found that the opening pressure is normal and CSF was clear and colorless using CT or MRI scan.
After laboratory examination for CSF sample, it is found that the white blood cells 400/mm3, neutrophils 15%, lymphocytes 85%, red blood cells less than 5/mm3, protein 0.6 g/L (normal > 0.4 g/L), CSF: serum glucose ratio 0.62 (normal 0.6). All bacterial tests were found negative.
The teenager’s mother tells the doctors that his sister, Germaine, has been diagnosed as having mumps. Her face has been swollen for 3 days and a number of her classmates also have mumps. Therefore, the doctor took two samples from the patient for diagnosis which are blood and CSF samples for antibody testing and mumps PCR respectively but the result was mumps negative.
On the 2nd day, the teenager’s condition appears to have worsened overnight. His headache is somewhat worse and he remains febrile (38C). He has also become drowsy and lethargic so that a repeating sample of CSF is requested but the neurologist advises against it until after the result of a CT or MRI scan is to become available because he wanted to be sure that there is no increased intracranial pressure. At this stage, intravenous acyclovir is given to the patient due to the progression of symptoms of the disease and we performed a PCR test on the same CSF sample that was obtained from the patient for herpes simplex virus but the result was also negative. On day three, the teenager’s health is starting to improve. His temperature is lowering and he is becoming more alert. Therefore, a PCR test was also performed on the CSF sample for detection of enteroviruses and the result was finally come out positive as shown in (Figure 1). Furthermore, the MRI result shows that it is likely to be normal. In the end, we performed a blast for the sequence provided to determine which genotype of the enteroviruses has caused the infection.
Severe aseptic meningitis with viruses is rare. There are only some documented cases of severe and progressive meningoencephalitis or encephalitis especially in the UK and the USA. By contrast, most of the cases have been described as mild viral meningitis particularly in adults and children and they may recover without being admitted to hospital [1]. Similar cases of infectious meningitis occur by other infectious agents mainly by bacteria. Although it is less common than viruses, the infection is often more severe and associated with a high risk of progression and high mortality rate [4-6]. The most common types of bacteria causing meningitis in the UK are Neisseria meningitides and Streptococcus pneumonia [5]. Less commonly, fungal meningitis may also occur in young adults but it is more frequent in immunocompromised patients [7].
Annually, viruses can cause a higher incidence of meningitis than that of other infectious agents particularly bacteria but it is usually less severe than them [4,6]. Differentiation of viral meningitis from bacterial one on admission to hospitals is based on clinical manifestations and laboratory tests performed mainly on cerebrospinal fluid (CSF) samples. This differentiation has significant benefits in reducing the usage of antibiotics and hospital admissions and it also assists inappropriate treatment of the infected individual and management of contacts [1].
Although enteroviruses are reported as a major cause of viral meningitis in developed countries, a number of other significant viruses are also known to cause meningitis (acute and chronic) as well as meningoencephalitis in children and adult. An important example of other viral meningitis and central nervous system (CNS) infections is the herpes virus family especially the herpes simplex virus (1 and 2) which is associated with high morbidity and mortality rate when the infection is progressed into encephalitis. Therefore, early treatment with acyclovir is necessary and can significantly reduce the disease complication, however, meningitis caused by herpes viruses is often self-limited and recover without treatment [3,8]. Furthermore, in recent studies in the UK, mumps virus has also reported as the commonest pathogen of meningitis in young adults, although it is usually mild and associated with low mortality rate, this might particularly be due to the presence of MMR vaccine against it, however, some studies have reported that the MMR vaccination itself may rarely associate with complicated aseptic meningitis [1,3]. Other significant pathogens are including measles, chickenpox, and some other viruses but because of the availability of vaccination programs against them particularly for measles and chickenpox viruses, today they can be prevented and they became a rare cause of viral meningitis [3].
Nowadays, enteroviruses are commonly known to be responsible for most cases of viral meningitis especially in the developed countries, and like other causes of viral meningitis, they have a specific seasonality and particular geographical distributions. In a temperate climate, they tend to occur in late summer and early autumn and they may transmit through contact with contaminated respiratory secretions or through the fecal-oral route [9].
Human enteroviruses are a large group of positive single-stranded RNA viruses that belong to the family of Picornaviridae and they are generally divided into 2 distinct classes: polioviruses (types 1,2 and 3) and non-polioviruses (echoviruses, coxsackievirus, enterovirus, and unclassified enteroviruses) [10]. Each of them is further subdivided into several serotypes and they can infect people of all ages [10,11].
Echovirus serotypes of 6, 9, 11, 13, 19, and 30 are identified as the predominant causes of enterovirus meningitis, mainly in the USA, the UK, and Australia. In the UK, echovirus serotypes 13 and 30 are described to be the commonest; however, most of the cases are mild and rarely resulting in hospital admission and diagnostic lumbar puncture. Coxsackie viruses A and B, mostly B has also been reported as one of the main causes of aseptic meningitis in children, whereas polioviruses are now endemic in many Central African and West Asian countries, however, sporadic cases still occur in some other areas of the world [1].
In our case, because the patient has developed clinical signs of meningitis, he initially treated with antibiotics for bacterial infections but later it is found that the bacterial tests were all negative so that we thought that he is more likely to be infected by viral meningitis, especially with mumps virus because her sister had mumps before. Therefore, in the beginning, we carried out mumps PCR on CSF sample, but it was negative as well. On the day later, because the patient’s condition has progressed and worsened overnight and he developed the signs of drowsiness and lethargy, we performed herpes simplex virus PCR, and the patient is started intravenous acyclovir treatment until the result to become ready but it was also negative. Finally, we found that the result is enteroviruses positive after the performance of enteroviruses PCR and then after, by blasting the genome sequence of PCR product generated by amplification of a 115bp fragment of the virus protein 1(VP1) gene in order to determine enterovirus genotype, and we found that the teenager was infected with type B enterovirus and serotype Echovirus 11.
Special thanks to the staff of Microbiology and Virology, University of Manchester, UK
No conflict of interest

![]()

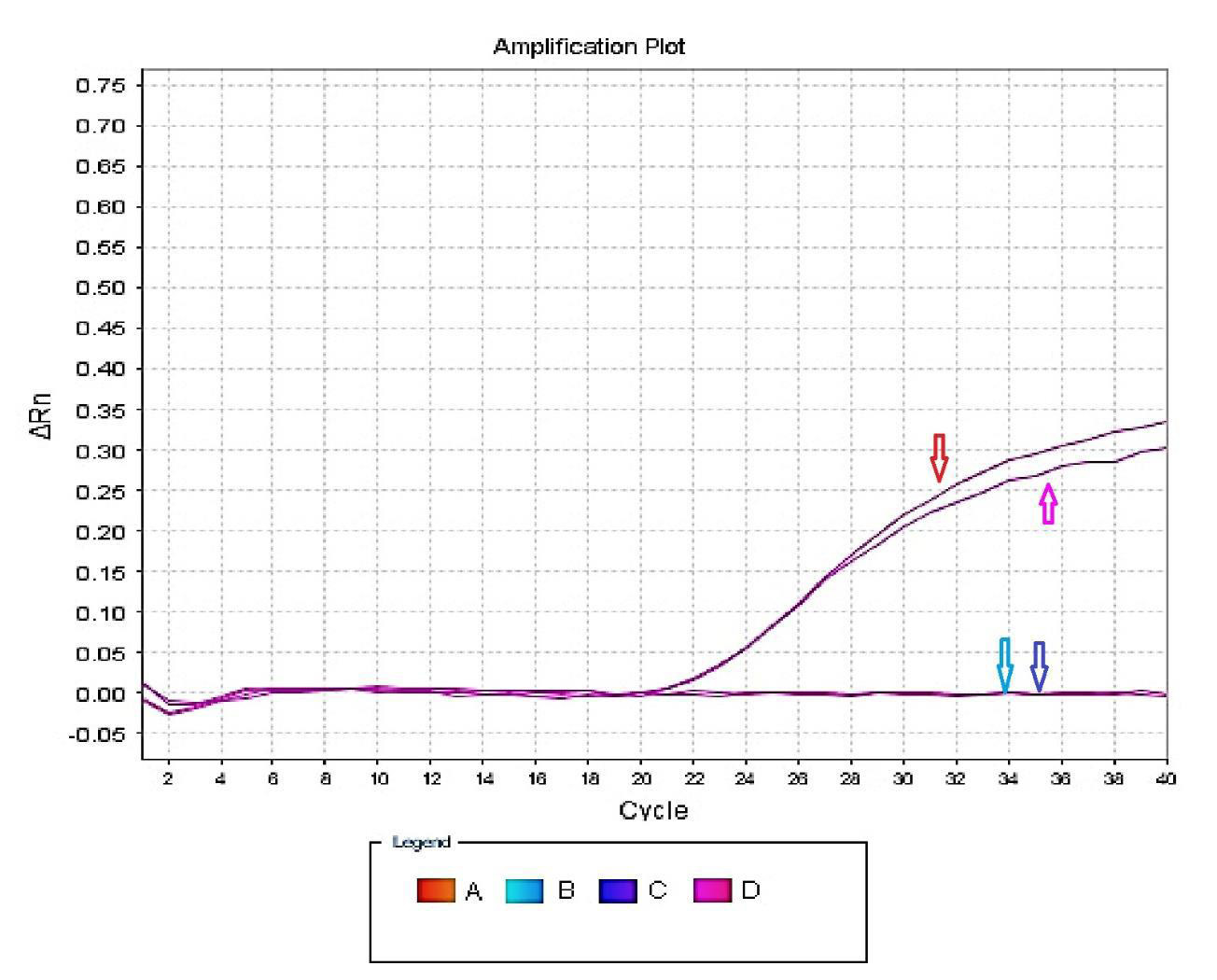 |
Figure 1: Real-Time PCR result of the patient's CSF samples; (A) CSF sample; (B) Negative sample; (C) Negative control; (D) Enterovirus positive control |




































