Open Access
Research Article
Max Screen >>
ISSN: 2394-6512
Copyright: © 2021 Ariff S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background: Enterovirus meningitis is one of the commonest viruses causing meningitis in children which is underdiagnosed. The epidemiology of EV infections is not well studied in the Middle East and Arab Gulf Region. No Study was conducted in Oman to explore more about viral meningitis. This study will help to review enterovirus meningitis in order to guide management and patient care in Oman and will help to decrease the cost of treatment by avoiding unnecessary investigations.
Aim and Rationale: This study demonstrates prevalence, clinical presentation and viral serotypes of non-polio enterovirus meningitis among Omani and non-Omani children less than 15 years admitted in Royal hospital; child health department during the time frame of 1/10/2015 to 29/04/2016. We also aim to increase awareness among paediatrician and general practitioners to have a low threshold of investigating children with typical presentation of enterovirus meningitis and to guide the management plan which will help in reducing the number of inpatient days and antibiotics usage.
Methods: A retrospective chart review study was conducted at Royal hospital, a tertiary care centre in Sultanate of Oman, during the period between 2015-2016. All clinical aspects were studied including clinical presentations, laboratory findings and outcomes.
Results: A 38 cases were included in the study with almost 60% males compared to 40% females. Among all symptoms studied, fever accounts for 87%, headache 66%, 52% had neck stiffness clinically and only 11% had bulging fontanelle. Among other symptoms, lethargy is the most common symptoms with almost 11%. Respiratory viral panel done in 87% of the patients and PCR was positive for enterovirus in 45% compared to CSF enterovirus PCR which accounts for 18.4%.
Conclusion: We conclude that enterovirus meningitis has wide range of clinical presentation. It is mild self-limiting infection in otherwise healthy children with fully recover. Most of the cases did not required prolonged antibiotics.
Keywords:Enterovirus; Meningitis; Children; Clinical Spectrum; Outcome
List of abbreviations: WBC: White Blood Cell; RBC: Red Blood Cell; PLT: Platelet; RVP: Respiratory Viral Panel; LP: Lumbar Puncture; PCR: Polymerase Chain Reaction; CSF: Cerebrospinal Fluid; CT: Computed Tomography; CRP: C Reactive Protein; EV: Enterovirus
Meningitis is defined as an inflammation of the leptomeninges caused by bacteria or viruses’ infection [1]. Viral meningitis is not uncommon but is less serious, and most of the time self-limiting. It is more severe in children less than one month of age and in the immunocompromised. However, it is very important to detect viral meningitis to rule out serious causes and to guide management plan.
Many viruses can cause meningitis. Among these are non-polio Enteroviruses which are single-stranded RNA viruses. There are almost of 100 serotypes under picornavirus family [2]. The main site of replication is lymphoid tissues in the gut and oropharynx that leads to viremia that last for 3-5days. After viremia phase; the viruses spread into other organs like lungs, CNS, heart and liver. The incubation period is around 3-6 days. Humans are the only natural host of enteroviruses. Transmission of infection is by faecoral and respiratory routes. 10-20 million of symptomatic infections per year in United State due to enterovirus. They are more prevalent among children because of multiple factors including crowding, poor hygiene, and opportunities for fecal contamination in lower social economic countries [3].
The Enteroviruses have a worldwide distribution, with marked summer/fall seasonality in temperate climates and high year-round incidence in tropical and subtropical areas. Viral RNA PCR is the mothed used to diagnosed enterovirus [4].
The epidemiology of EV infections is not well studied in the Middle East and Arab Gulf Region. In Saudi Arabia, there has been a significant increase in EVs during midwinter [5]. So far, no study was conducted in Oman to look for enterovirus infection among children.
This is a retrospective chart review study that looks into enterovirus infection in children, its clinical presentation, methods of diagnosis, outcome and further management that helps the paediatricians to have a wider scoop in management and better focused and cost-effective management plan.
This is a quantitative descriptive study. A retrospective chart review study that conducted at the Royal hospital tertiary care canter in Oman. Data were collected from electronic records of (Al-Shifa System) and transferred in data collection sheet using epi-data entry software. In this study we included all Omani and non-Omani children less than 15 years of age who admitted in paediatrics words of Royal Hospital from 1/10/2015 to 29/04/2016 with history of fever, headache, photophobia and phonophobia with positive non-Polio enterovirus in the respiratory viral panel or positive CNS multiplex PCR which differentiate it from Polio enteroviruses.
Exclusion criteria: children >15years of age, presence of other organisms in CNS culture or RVP.
For data analysis, SPSS program was used. For descriptive purposes, categorized variables was described as percentages. Continuous variables were presented as mean with standard deviation.
Before conducting this research, Ethical approval and permission was obtained from Royal Hospital Research Committee. Confidentiality was maintained throughout the research and the data were used for the research purposes.
Samples belonged to 38 children who were admitted in general paediatrics ward at the Royal Hospital, Muscat, Oman. Among 38 patients diagnosed with meningitis based on clinical presentations and laboratory findings, 60% (23 patients) were males and 40% (15 patients) were females. 92% of the cohort were Omani. Age range at time of presentation was from 1 month to 13 years. Median age of presentation was 7 years. 32% of them were under one year of age. All cases were presented to the hospital within winter season, and peak of cases was in January as shown in graph 1. Two methods were used for testing, Respiratory viral panel that was performed in 87% (33 patients) vs 13% (5 patients) no RVP PCR done. Lumbar puncture was done in 92% (35 patients) vs 8% (3 patients) family refused Lumbar puncture but the RVP PCR was positive in these three patients.
Duration of symptoms ranged between 2- 5 days before presentation to the hospital. Median duration of symptoms was 3 days before visiting the hospital is more prominent with 47% compared to other days 2, 4 and 5days with (24%, 24% and 5% respectively). Fever is the most common symptoms which accounted for 87% of symptoms then headache 66% and vomiting 60%. Median fever was 38c degree. Neck pain was only present in 47% of symptoms. Photophobia accounts for 26% compared to phonophobia 16%. Other symptoms were included in the study include lethargy, irritability, poor feeding, seizure, upper respiratory tract infection (URTI) symptoms, and abdominal pain. Among these symptoms, lethargy was more prominent in 4 patients (10.5%). Upper respiratory symptoms were only present in 5%. Among this cohort of children, only 34% were having positive history of contact with sick people. Out of all contact, only 5 patients were having sick contact in the hospital (~13%).
Clinical assessment of these children showed neck stiffness was positive in 53%, Kering’s sign is positive in 42% vs 55% were negative and not documented in 3%. Brudnizki’s sign is positive only in 24%, negative in 74% and 2% not documented. Bulging fontanelle only present in 10% (children less than 2years). Initial presentation to the hospital was of mild to moderate in severity for all admitted children and did not progress to severe illness during stay in general ward. Table 1 shows detailed clinical assessment of the admitted children.
On admission, complete septic works up was done including, CBC, CRP, urine culture, blood cultures, CSF analysis and respiratory viral panel. Serum glucose level and platelets count were within normal range, only one child was having low blood glucose on presentation. Few cases were having slightly elevated platelet counts 2% of the total cohort. Details of all blood works up and CSF results are shown in tables down.
CRP in most of patients was almost ~79% within normal range in initial presentation to the hospital (CRP 5mg/dl), but around 21% were slightly above normal range. Serial CRP during admission, showed 12% raised of CRP levels that normalized before discharge. Blood cultures were sent in all patients. 100% of them were negative cultures for bacterial growth. Respiratory viral panel was done on 87% among the cohort. Out of total 33 samples of RVP, 17 samples were positive (~45%), 15 samples were negative (~40%) and 6 samples (~15%) were not processed due to samples leak while transporting them to the lab for analysis. Urine culture was done and all negative in all 38 patients.
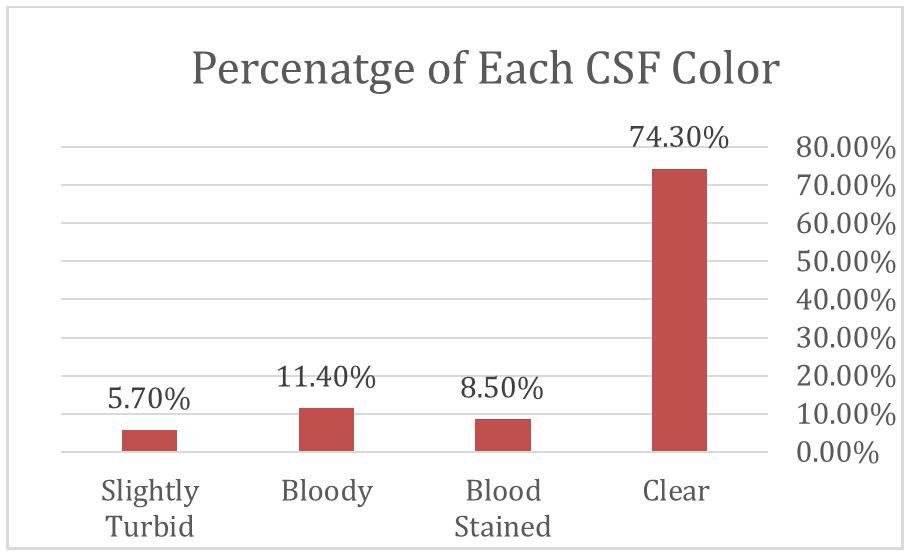
Lumbar puncture was performed on 35 patients (92%) compared to 3 patients (8%) as family refused the procedure. This percentage of lumbar puncture performed in this cohort was considered significant in view of wrong belief of the families regarding LP and high refusal rate in general. We noticed that in 74.3% of LP samples, CSF fluid was clear compared to 11.4% of bloody CSF and 5.7% of slightly turbid CSF as shown in graph.2. In 92% of the patients where LP was done; CSF cultures were negative vs 8% without results as LP was not done. CSF viral PCR was done in 32% of CSF samples. Around 19% were positive of enterovirus vs 19% were negative with CSF enterovirus. In 62% CSF virology PCR were not done due to technical issues in virology lab.
CT scan was done in around ~ 16% of patients mainly in those with prolonged recovery time > 3 days, looking for any CNS complications. All CT scans were done in older children. All CT scans were normal except one child (3%) with leptomeningeal enhancement. No brain MRI was done during this study period. None of the children required follow up brain imaging.
53% of the patient received antibiotics treatment for total of 10 days vs 32% for 7days. Only 2% received treatment more than 10 days. Median length of hospital stays was calculated as 9 days., Empirical antibiotics were continued after the results of the CSF viral PCR result as enterovirus infection was thought to be coinfection with other bacterial infection. 66% of the children received only empirical ceftriaxone from the time of admission. 16% received both ceftriaxone and acyclovir. And almost 11% received ceftriaxone and vancomycin (graph no.3). None of them required anti-epileptic medications. No admission in intensive care unit during stay in general wards. All patients had full recovery without any sequels. Average recovery period between 3-5 days after admission.
This study provides details about clinical presentation and laboratory findings of enterovirus meningitis among 38 children admitted at tertiary care centre. The bulk of the patients presented to our centre at one time during winter season 2015, which is not commonly reported during the winter season time where other studies showed peak of enterovirus infection during summer. However, we could not study seasonal variation of the disease as only few cases presented after winter season.
In literatures, enterovirus was known to have high morbidity and mortality in pediatrics age groups, especially neonate and infants less than one year of age [6]. But recently, these morbidities and mortalities became less. Like other studies, enterovirus can present at any ages. It is common to have severe infection in neonate, mainly less than two weeks of age. None of our population were less than 2 weeks, so most of them were having mild to moderate course of the disease. Meningo-encephalitis was commonly caused by enterovirus. It has being reported that three different manifestations were associated with higher mortality associated with enterovirus infection like myocarditis, hepatitis and coagulopathy [7]. The good outcome of this cohort might point to less invasive enterovirus causing meningitis. Another reason could explain that most of our study’s population were aged more than one year (~ 68%) and all of them without any co-morbidities.
Older children were presented with classical meningitis like picture with fever, frontal headache, vomiting and more of photophobia compared to phonophobia. Lethargy were most common in neonate and infant. But fever is the prominent symptoms among both groups’ neonate and older children. Another interesting finding noticed in this study that respiratory symptoms were seen in only 5% but respiratory viral panel was positive of enterovirus in 45% of samples. Also, most of the history of contact was of meningitis symptoms rather than respiratory symptoms. We found that from our cohort 5 patients were family members, two were cousins and three of them were siblings.
Clinical assessment, like other older children, both neck stiffness and kering’s sign were seen in patient with enterovirus meningitis. Younger children were having unspecific findings on assessment ranging from (lethargy, bulging anterior fontanelle and clinical seizure). Other systemic examinations were unremarkable [8].
Even though, there was a different range of total white blood cell counts according to age. In our study, older children have lower or normal blood white cell counts (WBC) compared to children less 1 year with high WBC in the blood. Among differential counts, lymphopenia was noticed in children > 1year of age. All patients less than 1 year of age, presented with either normal or high lymphocytes counts. These findings might give a clue regarding viral infection. CRP levels were initially normal in initial presentation; few cases were having slightly high CRP > 5 mg/dl that improved before discharge. In literature, Enteroviruses are transiently present in the CSF during acute infection, but still with that we got 19% positive PCR out of only 32% of samples were sent. CSF pleocytosis count was also varied according to age. In general, children less than 1 year of age were more likely have higher WBC counts in CSF compared to older children who have lower or just slightly higher CSF pleocytosis. Most of CSF samples showed higher lymphocytes in CSF compared to polymorphs in both age groups that was recorded as percentage in CSF microscopy. CSF protein were also less in both groups and CSF glucose were normal in CSF.
Radiological investigations in term of imaging is only limited to small number of patients with meningitis in general [9]. In our study, CT scan was justified in patients who required prolong time to recover despite being on treatment. Out of 6 patients who had head CT, only one child was having meningeal enhancement.
Most of these children had very good recovery 3 days during admission. Fever remained only up to 48 hours after admission. Most of them were returned to normal baseline of their activities. It had been observed that at initial peak of illness these children were treated aggressively with antibiotics and acyclovir as there was initially no clear clue of enterovirus infection. later as most of RVP and CSF virology PCR was positive to enterovirus. Some of them were continued on antibiotics regardless of the result for average of 10 days waiting for the CSF and or blood culture. But later after the initial number of patients; there was a total change in practice of antibiotics duration and duration of admission as these children got diagnosed based on clinical presentation and increased number of cases of enterovirus infection during the study period. None of our patients required anti-epileptics medications on discharge. This cohort had excellent outcome with 100% of children had full recovery. None of our patients were re-admitted again within after discharge with same complains.
This is the first single centre study performed in Oman to review cases of enterovirus infection in children. All cases were presented with aseptic meningitis and CNS symptoms that mostly seen in pediatrics age group. Clinical presentation can vary between age groups, but no severe cases were reported in our group of patients compared to other studies. Knowing the clinical presentation, blood, respiratory viral panel and CSF investigations helps to early diagnosis of enterovirus meningitis and avoid unnecessarily antibiotics use and cost investigations and help in expecting the outcome and counselling the parents.
We recommend multicentre study that looks to enterovirus infection in children. It is also important to study this infection over years to look for seasonal variations in the country. Further testing is required to identify serotypes and correlate them with severity of the illness. If there is a suspicion of enterovirus infection based on clinical extent, we recommend widening the laboratory testing of blood, respiratory, CSF, stool and urine for more reliable results. Earlier respiratory, stool and urine results might guide the paediatricians to discontinue antibiotics early and safely. We recommend that frequent neurodevelopmental follow up of the children with enterovirus meningitis to look for any long-term sequel of this infection.
There are number of limitations in this study. First, it is a retrospective study with potential bias due to missed information. Second, small sample size is one of the major limitations. Third, stool samples were not tested in these patients that might add also to this study’s result. Another limitation to the study was technical issue in the laboratory which resulted in limited testing of the CSF for enteroviruses in some of the patients. Refusal of lumbar puncture by families is another limitation but RVP test were used instead which can give indirect link to the cause of enterovirus meningitis. Also, we could not test which serotype of enterovirus is most common as still further testing is required and giving limited resources it was not done for this cohort. In addition, neurodevelopmental follow up of these patients was limited which could miss long term sequel of enterovirus meningitis.

![]()

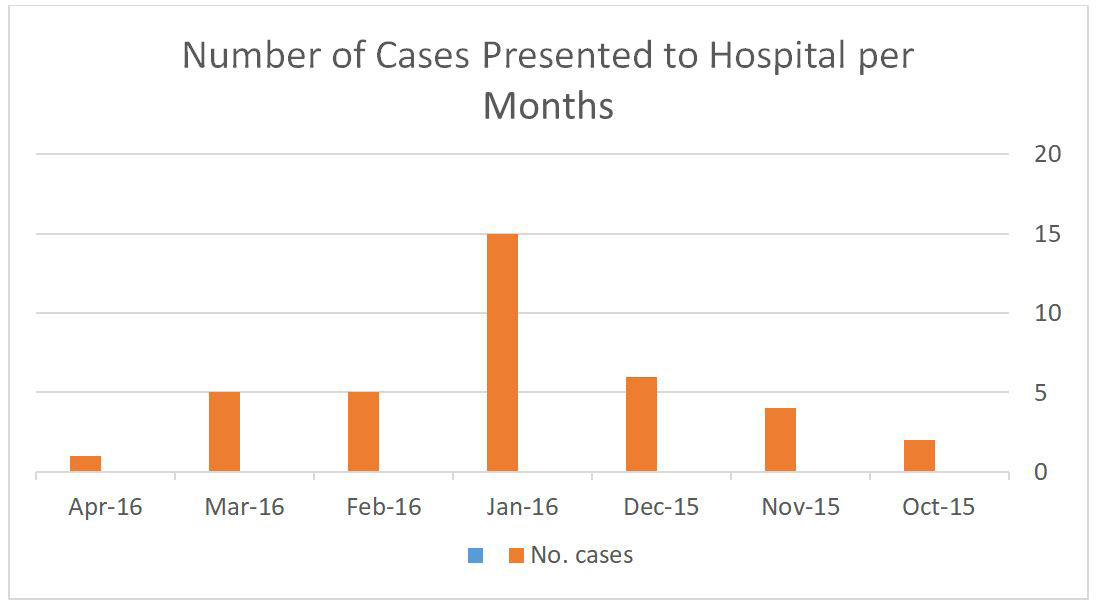 |
Graph 1: Number of Enterovirus Cases Per Month Admitted to Hospital with enterovirus meningitis |
Clinical Features |
Total (n= 38) |
Age =< 1 year (n=12) |
Age > 1 year (n= 26) |
At Presentation |
|||
Fever n (%) |
33 (87%) |
7 (58.3%) |
26 (100%) |
Temp, Median (IQR) |
38 (37.5C-40C) |
38 (37.6C-39C) |
38 (37.6C-40C) |
Headache, n (%) |
26 (68.4%) |
0 (0%) |
26 (100%) |
Vomiting, n (%) |
23 (61%) |
3 (25%) |
20 (78%) |
Neck Pain, n (%) |
18 (47%) |
0 (0%) |
18 (69.2%) |
Phonophobia, n (%) |
6 (16%) |
0 (0%) |
6 (23.1%) |
Photophobia, n (%) |
10 (26%) |
0 (0%) |
10 (38.5%) |
Lethargy, n (%) |
3 (7.9%) |
3 (25%) |
0 (0%) |
Irritability, n (%) |
4 (10.5%) |
4 (33%) |
0 (0%) |
Poor feeding, n (%) |
3 (7.9%) |
3 (25%) |
0 (0%) |
Seizure, n (%) |
1 (2.6%) |
1 (8.3%) |
0 (0%) |
URTI, n (%) |
2 (5.3%) |
2 (16.6%) |
0 (0%) |
Abdominal pain, n (%) |
3 (7.9%) |
0 (0%) |
3 (11.5%) |
History of Contact, n (%) |
13 (34%) |
5 (42%) |
8 (31%) |
Capillary Refill Time > 2sec- onds, n (%) |
24 (63.1%) |
7 (58.3%) |
17 (65.4%) |
Tachycardia per age, n (%) |
20 (52,6%) |
6 (50%) |
14 (53.8%) |
During the Course of the Disease |
|||
Fever, n (%) |
28 (73,7%) |
8 (66.7%) |
20 (77%) |
Duration (days), Median (IQR) |
2 (1-3) |
2 (2-4) |
2 (1-2) |
Peak Temperature, (c), median (IQR) |
38.6 (38-40) |
38.7 (38.1-39) |
38.3 (38-40) |
Table 1: Detailed Clinical Assessment of Admitted Children
Statistics |
Hemo- globin (in gm/ dL) |
WBC(in x 10^9 per L) |
Neu- trophilis (in x 10^9/L) |
Lympho- cytes (in x10^9/L) |
Plate- lets (in x10^3/ ul) |
WBC |
RBC |
Poly- morphes (in percent- age) |
Lym- phocytes (in percent- age) |
Protein in CSF bio- chemistry (g/L) |
Glucose in biochem- istry of CSF (in mmol/L) |
Random blood sugar (in mmol/L) |
Total |
38 |
38 |
38 |
38 |
38 |
35 |
35 |
35 |
35 |
35 |
35 |
38 |
Mean |
11.95 |
11.03 |
6.96 |
2.97 |
312.50 |
49.00 |
1447.2 |
19.53 |
43.58 |
.29 |
2.79 |
4.98 |
Median |
11.65 |
10.40 |
5.55 |
1.90 |
291.00 |
24.00 |
3.00 |
10.00 |
50.50 |
.26 |
3.20 |
4.90 |
Std. Deviation |
1.79 |
5.24 |
4.46 |
2.60 |
91.26 |
102.19 |
8102.6 |
23.73 |
38.15 |
.26 |
1.69 |
1.31 |
Minimum |
8.20 |
3.80 |
1.30 |
.50 |
170 |
2 |
2 |
0 |
0 |
.00 |
.00 |
2.10 |
Maximum |
16.10 |
29.70 |
19.20 |
9.40 |
585 |
612 |
50000 |
80 |
97 |
1.20 |
5.50 |
7.80 |
Table 2: Full blood count and cerebrospinal fluid parameters
|
Graph 2: Percentage of Each CSF Color |
Laboratory Tests at Presentation |
|||
Labs Parameters |
Total (n=38) |
Age =< 1 year (n=12) |
Age > 1 year (N=26) |
WBC counts, (/ul), median (IQR) |
10.4 (3.8-16.1) |
9.8 (5.3-16) |
9.2 (3.8-29.7) |
Low WBC counts, n (%) |
13 (34.2%) |
10 (83.3%) |
3 (11.5%) |
Raised WBC counts, n (%) |
6 (15.8%) |
2 (16.7%) |
4 (15.3%) |
Lymphocytes (/uL), median (IQR) |
1.65 (0.5-9.4) |
4.65 (1.7-9.4) |
1.55 (0.5-3.9) |
Low Lymphocytes counts (/uL), n (%) |
23 (60.5%) |
5 (41.6%) |
18 (69.2%) |
Raised Lymphocytes counts (/uL), n (%) |
0 (0%) |
0 (0%) |
0 (0%) |
Platelets counts (/uL), median (IQR) |
280 (170-585) |
357(241-585) |
282 (170-478) |
High PLT Counts, n (%) |
8 (21.1%) |
3 (25%) |
5 (19.2%) |
Low PLT Counts, n (%) |
0 (0%) |
0 (0%) |
0 (0%) |
CRP (mg/L), median (IQR) |
3 (1-60) |
4.5 (1-60) |
4.5 (1-40) |
CRP < 5 mg/L, n (%) |
30 (78.9%) |
8 (66.6%) |
22 (84.6%) |
CRP >= 5 mg/L, n (%) |
8 (21.1%) |
4 (33.3%) |
4 (15.4%) |
CSF Parameters |
|||
CSF cell Counts (/uL), median (IQR) |
40 (0-612) |
40 (0-612) |
47 (6-200) |
CSF Pleocytosis, n (%) |
30 (78.9%) |
8 (66.6%) |
22 (84.6%) |
Polymorphes in CSF (%), median (IQR) |
20 (0-80%) |
20 (0-50%) |
30 (0-80%) |
Lymphocytes in CSF (%), median (IQR) |
58 (0-97%) |
53 (0-90%) |
59 (0-97%) |
CSF Protein (mg/L), median (IQR) |
0.30 (0.14-1.20) |
0.29 (0.14-0.84) |
0.32 (0.19-0.8) |
Raised CSF Protein (mg/L), n (%) |
8 (21.1%) |
3(25%) |
5 (19%) |
CSF Glucose (mg/dL), median (IQR) |
3.7 (2.5-5.5) |
3.3 (2.7-5.1) |
3.7 (2.5-5.5) |
Low CSF Glucose, n (%) |
16 (42.1%) |
6 (50%) |
10 (38.5%) |
Serum Glucose (mmol/L), median (IQR) |
4.5 (3.2-6.3) |
4 (2.7-5.4) |
5.15 (2.1-6.8) |
Low serum Glucose (mmol/L) |
5 (13.1%) |
3 (25%) |
2 (7.7%) |
WBC (White Blood Cells), RBC (Red Blood Cell), IQR (inter-Quartile Range), CRP ( C Reactive Protein), CSF (Cerebrospinal Fluid), PLT (Platelets)
Table 3: Detailed CBC and CSF Parameters
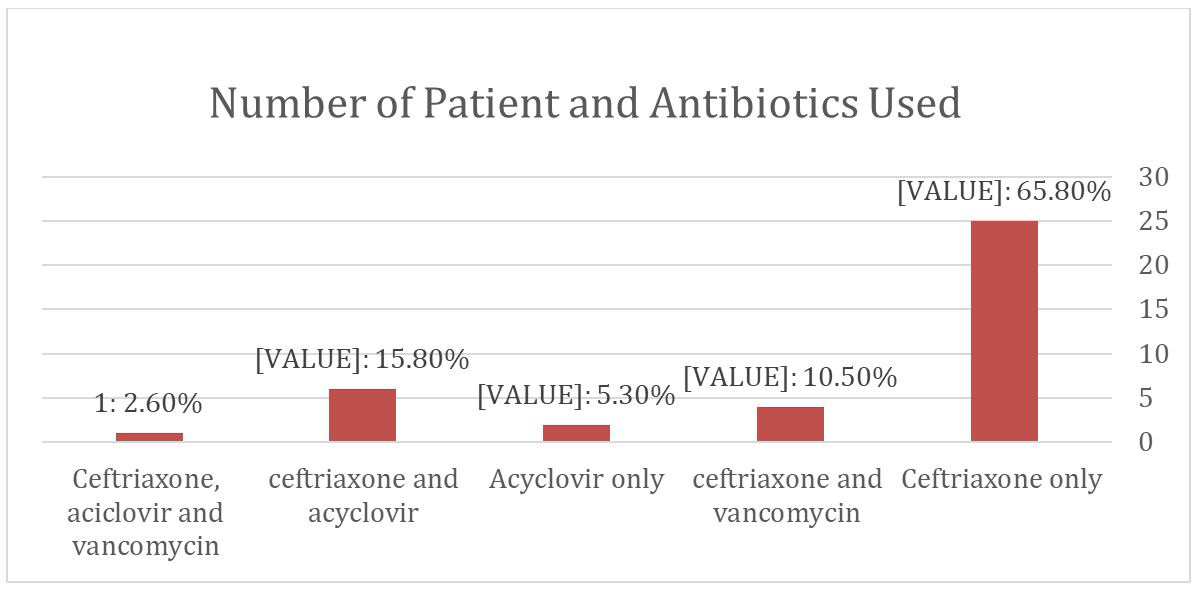 |
Graph 3: Number of Patient and Antibiotics Used |