Open Access
Research Article
Max Screen >>
ISSN: 2348-9804
Copyright: © 2021 Ariff S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
A growing body of evidence gathered over the past 10 years has demonstrated a clear escalation of sudden death (SD) in Chinese medical staff. This retrospective study was conceived to explore the first evidence of signs of SD, relieving clinical workload and strengthening protection against the overload of Chinese medical staff. A systematic search of public reports on medical and authoritative Chinese websites, official documents and in articles published in PubMed, Web of Science and ProQuest databases between January 1, 2008 and August 30, 2018 was undertaken. In addition, data from the Chinese National Health and Family Planning Commission report was also analyzed. Over this time period, 109 sudden death occurrences with a 2.75% rate of rescue were reported for Chinese medical staff due to overwork, of young Chinese physicians aged 39.72 ± 9.39 years (male: 40.43 ± 9.14 years; female: 33.73 ± 9.77). The ratio of males to females was 8.36 : 1. Most were surgeons (40.37%), anesthetists (19.27%) or internists (16.51%) principally located within developed regions in China. Among these 109 incidents, 78 were confirmed to be in specific locations. Sixty-seven (85.90%) occurred within hospital or at home. Confirmed causes of death included cardiac arrhythmia, dissecting arterial aneurysm and rupture of cerebral blood vessels while many had no apparent abnormality at autopsy. It is essential to relieve clinical workload and strengthen protection against the overload of Chinese medical staff beyond the forthcoming emergency rescue for SD.
Schematic view of ideal measures for the prevention of karoshi relating to the present study from external and internal points-of-view. A rational preventive framework includes integration of the establishment of medical labor law, consummation of the hierarchical medical system, optimization of promotion and development of the doctor-patient relationship, viewed from an external point-of-view. Chinese medical staff attending to their own health relates to an inside point-of-view on behalf of Hippocrates of Cos.
Keywords:Sudden Death; Physicians; Stress; Burnout; Medical Staff; Public Health
Doctors are the essence of our civilized world. - Robert Lewis Balfour Stevenson (1850-1894)
Since the promulgation of the revised Physician’s Pledge (8th edition) [1], protection of the health of physicians has been recognized globally. When the health of medical staff in China was more closely inspected, it has become clear that the continual incidents of sudden death (SD) constitute the greatest challenge for Chinese medical staff [2-4]. Besides the physical and verbal violence perpetrated against doctors [5,6], overwork-induced SD, a non-violent and otherwise unexplained death occurring within 24 h of the onset of symptoms [7], is an additional threat. In particular, a number of contradictions within the Chinese medical environment have caused a reduction in the gross capacity of medical staff and increasing numbers of medical graduates preferring not to take up medical posts [8,9]. Such a tendency for the loss of staffing capacity is a serious situation, considering the explosive growth in demand for medical resources. Thus, the emergence of overloaded medical staff facing high practice costs and risks has become a public secret in the Chinese medical industry. Ironically, most medical workers lack sufficient energy to consider their own health under the high pressure of workloads.
However, occasional reports describing SD in Chinese medical staff have not improved the situation even though a revised Declaration of Geneva has been published by the World Medical Association. For example, the Chinese National Health and Family Planning Commission yearbook, published on January 9, 2018, indicated that Chinese physicians worked more than 50 hours per week, far above the forty hours required by national labor law, negatively correlated to their professional level [4]. Nearly a quarter did not enjoy regular holidays and had inferior remuneration to physicians in Europe and the USA. Growing evidence further demonstrated that 33.2% of the physicians investigated suffered from at least one type of disease (hypertension, hyperglycemia, hyperlipemia, etc.[10]). Although many medical staff experience feeling at the brink of death, 39.6% did not attend their annual health check-up.
This phenomenon has become doubly harmful for the doctor–patient relationship, as SD not only results in the loss of medical resources and increased risk of medical service negligence [11], but also damages the integrity of the relationship between the doctor and patient and the harmony of the medical environment. Thus, disclosure of the patterns of occurrence of SD (incidence, regional distribution, specialties, incident black spots, temporal patterns, causes, successful rescue efforts and outcome) is of great importance for Chinese medical staff under high psychological pressure, intensity of work and therapeutic risks. Our first aim was to determine whether the incidence of sudden death for Chinese medical staff had increased during the period 2008 - 2017. SD Data, namely number of SDs and their regional distribution, victim specialty and incidence black spots were analyzed by correlation analysis. Secondly, to determine whether the occurrence of SD was related to specific temporal patterns, we performed a correlation analysis between numbers of sudden death incidents and the times they occurred (quarter, month and day). Thirdly, the causes, the success of rescue efforts and outcome of SD incidents were also investigated (Figure 1). This retrospective study was conceived to explore the first evidence of signs of SD, relieving clinical workload and strengthening protection against the overload of Chinese medical staff, at least via optimization of medical resource distribution.
Following approval by the Institutional Review Board of the Third Military Medical University Medical University for this study, a systematic search of public reports on Chinese authoritative websites (Xinhua News Agency, China News Service, China Daily, People’s Daily), medical websites, in official documents and in published articles referenced in China National Knowledge Infrastructure, PubMed, Web of Science and ProQuest between January 1, 2008 and August 30, 2018 was undertaken using the search terms: ‘medical staff’ Karoshi’, ‘doctors’ Karoshi’, ‘physicians’ Karoshi’, ‘anesthesiologists’ Karoshi’, ‘medical staff’ sudden death’, ‘doctors’ sudden death’, ‘anesthesiologists’ sudden death’ and ‘physicians’ sudden death’. In addition, data from the Chinese National Health and Family Planning Commission reports and yearbooks published by the government of China in 2017 were also analyzed to assure accuracy and completeness of the selected data during this 10-year period. These sources covered all of China. Only deaths listed in these articles or reports with complete information were included in this study. Cases where medical staff survived or private reports of death were excluded from the present study. Searches included appropriate wildcards and truncation. These sources covered all of China.
The recruited reports were identified through the electronic search. The title and the fulltext were reviewed on papers that were deemed potentially relevant. Finally, twelve combined records after duplicates removed were selected from China National Knowledge Infrastructure, PubMed, Web of Science and ProQuest between January 1, 2008 and August 30, 2018. Eighty-four reports on Chinese authoritative websites (Xinhua News Agency, China News Service, China Daily, People’s Daily), medical websites, in official documents were utilized. Finally, 109 subjects with SD among Chinese medical staff were selected (Figure 1). These publications were utilized for data analysis of incidence of SD, age distribution, geographical distributions of SD cases, physicians’ specialty, incident black spots, temporal patterns, causes, successful rescue efforts and outcome of SD cases.
The data for all victims in this study were recorded as mean ± standard deviation. All statistical calculations were conducted using SPSS20.0 statistical software for Windows. Correlation analysis was performed for all continuous variables and Chi-Square tests for categorical variables. Descriptive statistical methods were also used including percentages and proportions to describe categorical variables. Values of P 0.05 were considered significant. All P values were calculated as 2-tailed.
Among the SD incidents in this study, 103 victims were allocated into the study, except 6 of unknown age or gender. Their mean age was 39.72 ± 9.39 years (95% confidence interval [CI], 37.88 - 41.55). Of these, 92 were male with a mean age of 40.43 ± 9.14 years (95% CI, 38.54 - 42.32), and 11 were female with a mean age of 33.73 ± 9.77 years (95% CI, 27.16 - 40.29) (range: 20 years to 57 years) (P 0.01). The ratio of males to females was 8.36 : 1. Among these medical staff, 43 were surgeons aged 39.83 ± 8.73 years (95% CI, 37.15 - 42.53), 21 were anesthesiologists aged 36.05 ± 9.90 years (95% CI, 31.42 - 40.68) and 19 were doctors of internal medicine aged 40.47 ± 9.78 years (95% CI, 35.76 - 45.19) (Figure 2A,B,C and D).
Identification of region-specific SD of medical staff within the broad land area of China could ensure high grade protection. The results clearly showed that the areas with a sizeable number of victims were Jiangsu (12, 11.01%), Beijing (11, 10.09%) and Anhui (9, 8.26%). Deaths were also distributed within a number of provinces of Southeast and South China (Fujian, Guangdong, Shanghai and Zhejiang), plus a further one inland provinces (Henan) (Figure 3). The number of incidents was related to the level of regional gross domestic product (GDP) and work hours.
Results showed that SD mainly occurred within surgery, anesthesia and internal medicine departments, with 40.37% (43/109), 19.27% (21/109) and 16.51% (19/109) respectively, representing 75.70% (81/107) of all deaths (Figure 2E).
Among these 109 incidents, 78 were confirmed to be in specific locations. Forty-nine (62.82%) occurred within a hospital while 18 (23.08%) were at home. Ten (12.82%) victims were doing exercise (walking and body building), while one (1.28%) was drinking tea in a restaurant (P 0.01) (Figure 2F).
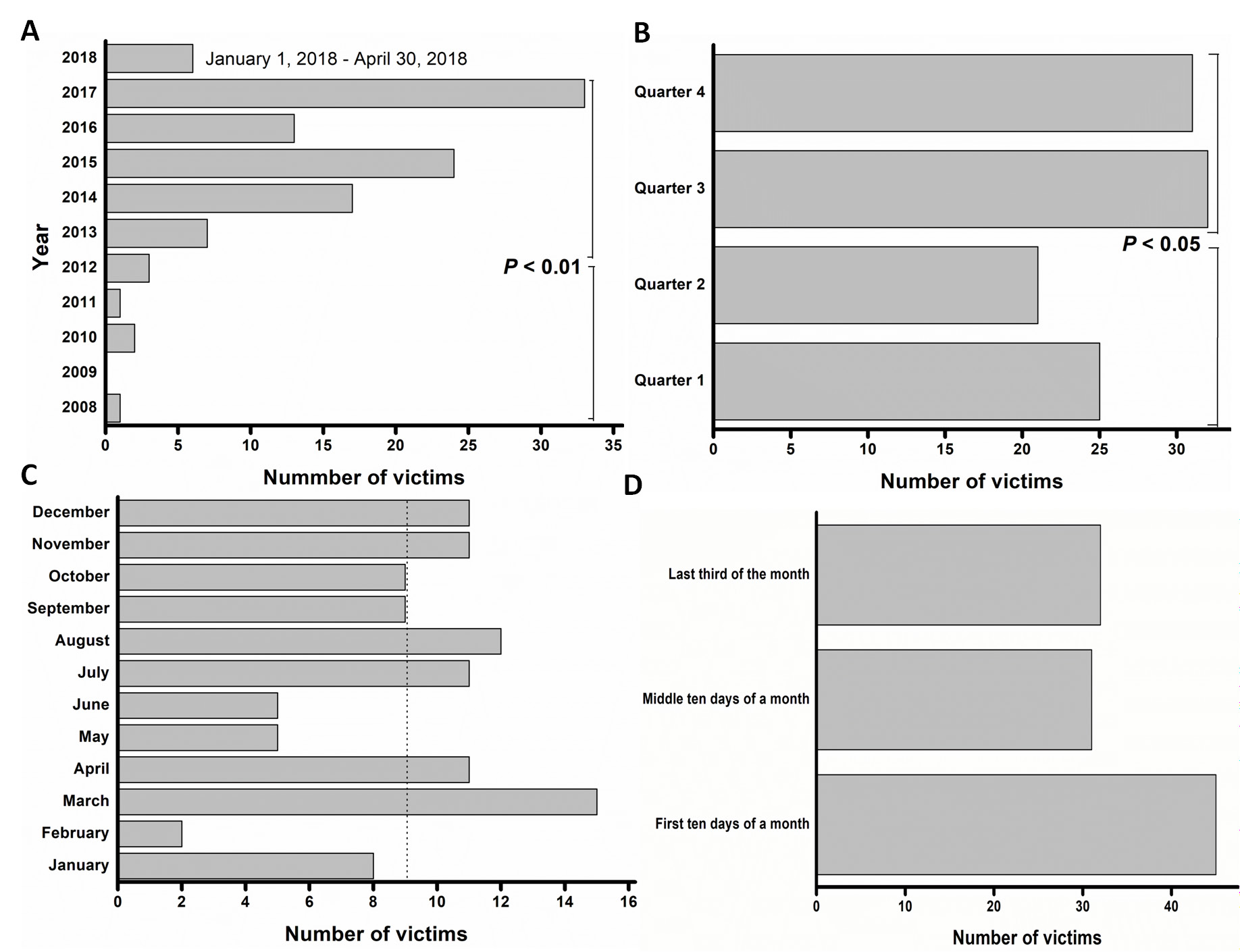
Further investigation was performed to clarify the possible temporal patterns for the high incidence of SD. Results indicated that the number of SDs escalated during the years under investigation. Between 2008 and 2012, the total number of deaths was 7 compared to 94 between 2013 and 2017, a 12-fold increase. Furthermore, a seasonal variation was observed, a larger number occurring in the third and fourth quarters (57.80%) compared to the first and second (P 0.05, P 0.01) (Figure 4).
Results further indicated that the SD in 94.50% (103/109) of victims had clear causes. All were overworked and suffered from overtiredness. In particular, consecutive work patterns, such as performing 40 cataract operations per day, medical treatment of 67 children followed by the saving of 3 severely unwell children in one night, or 48 hours of continuous duty, finally resulted in their demise. Also, 40 (36.70%) cases had confirmed causes of death. Of these, 37 (92.50%) suffered cardio-cerebrovascular accidents (cardio-cerebrovascular embolism, angiorrhexis for dissection of aorta and aneurysm). The remaining three died of septic shock, tumor and eye disease. Sixty-nine had no confirmed cause of death or apparent abnormality at autopsy. In addition, only 3 (2.75%), having occurred within a hospital (an operation room, department of anesthesiology or surgery), were saved while the other 106 died.
Compelling evidence over the previous 10 years has witnessed the number of cases of sudden death in Chinese medical staff clearly escalating. China consumes only 2% of the World’s medical resources although it has 22% of the global population [3]. This study underlined the incidence and outcome of SD among Chinese medical staff. We found that between January 1, 2008 and August 30, 2018, 107 sudden death incidents of Chinese physicians with a 2.75% rescue rate occurred due to stressful overwork, possibly the tip of an iceberg regarding their health status. SD occurred principally in young male Chinese physicians, mostly surgeons, anesthetists or internal medics, mainly within the developed regions with high population density in China. Furthermore, an analysis of the principal causes of SD demonstrated it was due to cardiac arrhythmia, dissecting arterial aneurysm and rupture of cerebral blood vessels [12-14], although clear at the time of death in this overworked cohort [14], many had no apparent medical abnormality.
Medical staff burnout is a worldwide problem [15,16]. The reasons for the upward trend in sudden deaths in Chinese young adult doctors can be explained as follows. Firstly, the current hierarchical medical system is unsound combined with a great shortage of physicians and lack of medical resources, especially for surgery and operative care. The demand from the Chinese public forces physicians to overwork in outpatient and inpatient treatments. Under this framework of overwork, average working hours described in the Chinese white paper in physician’s practice conditions in 2017 of 50.9 and 49.79 hours per week for male and female physicians, respectively, is not legally prohibited. The criteria for overwork-related diseases and deaths [14] are not generally recognized. More Chinese physicians need to take the statutory annual leave enjoyed by those in developed countries. However, even in Japan, many public hospitals do not regard physician’s night and holiday duties as work hours, further indicating that this field is highly competitive.
Secondly, the promotion schema for Chinese physicians sets seemingly universal criteria of National Science Foundation funding and articles published in Science Citation Index (SCI) journals [17,18]. Such dissociation between work and evaluation induces a burnout working pattern of 5 + 2 days plus day and night work. Long working hours and excessive work stress constitute an idiopathic killer [19]. Indeed, many young SD physicians seemed healthy. Previous autopsy findings also revealed that the majority of SD victims aged 1 - 45 years died from a cardiac disease. But a large number of deaths caused by circulatory diseases have not been recognized and have been reported as an undetermined cause for lack of a solid explanation for death [20]. Also, the occurrence of a sudden cardiac arrest due to structural heart disease is uncommon in young, healthy people [21]. Among these ascertained deaths, 13.16% of victims were doing exercise. Previous studies have revealed that sports activity is associated with a small risk of sudden cardiac death, predominantly in males [13]. Cardiovascular health and fitness should be considered important determinants, especially in overloaded medical staff [22]. Additionally, other work-related health problems, including insomnia, fatigue, gastric ulcer, and hypertension were easily seen in the high-pressure population.
Thirdly, the deterioration in the patient-doctor relationship resulted in Chinese physicians being wounded, disabled or killed by mentally-ill patients [5,6,23] or their relatives. A complex spectrum of diseases, greater surgical risks, and increasing numbers of complications further add to their workloads in addition to the shortage of doctors [24]. Thus, high work demand and a high-pressure work environment were always the major complaints in Chinese doctors. All these factors have resulted in persisting stress causing an extreme release of stress hormones and chronic inflammatory and immune responses [25]. Also, incorrect stress relief manners (excessive alcohol consumption, smoking, and long-term energy drink consumption) also affect physicians’ health [26]. A meta-analysis among 603,838 men and women from 24 cohorts in Europe, the United States, and Australia showed that SD from overwork is often caused by stroke and is believed to result from a repetitive triggering of the stress response [27]. The systemic exhaustion resulting from such stress might explain the deaths from heart attacks with no pathological findings. Also, these associated factors are inter-related.
Meanwhile, a 12-fold increase in SD of Chinese doctors between 2013 and 2017 than between 2008 and 2012 indicated that there was lack of sufficient measures against the serious outcome especially for young adult surgeons, anesthetists, and internists in these ten years. Also, region-specific SD of medical staff in China indicated that high grade protection is required especially in developed provinces. Incident black spots showed that 62.82% of incidents occurred within a hospital especially in March and August, Quarter 3rd and 4th, and first ten day of a month, meaning that most of them were on the edge of burnout at this moment when the incidents occurred. The narrow escape of SD among them could only be seen in an emergency unit within a hospital to date.
An improvement in the health of overloaded Chinese medical staff is urgent. The hierarchical medical system needs to be dismantled so as to enable the rapid redevelopment of primary medical care and medical resource redistribution, especially under the medical treatment alliance. Receiving promotion and social benefits should be accommodated within the clinical practice of Chinese physicians [3,4,18]. In addition, the task of attracting more medical graduates to enter the profession after qualification may fill the huge gap in vacancies. Since the law on the Prevention and Treatment of Occupational Diseases does not include SD-related cardiovascular diseases in mainland China [28], a compulsory furlough system is required [29], rather than violations of labor laws [11], for the most heavily-loaded Chinese medical staff, especially under a legal framework or through a central government initiative [30]. Additionally, public welfare and medical treatment could be coordinated within a government structure, through insurance or by individual’s payments, while the rational decoupling of remuneration and medical service may relieve excessive workloads for Chinese physicians.
Additionally, regarding concerns about sudden death, an internationally-recognized work-related hazard [31], the susceptible gene for SD [32,33] may be genetically screened to supply a prewarning indicator for those overworked medical staff in the future studies. If the carrier of a susceptible SD gene is identified as being potentially at risk, a decision could be made to provide appropriate occupational planning in clinics. Meanwhile, physicians should receive a regular health examination concerning the self-rated health measurement scale [34]. Recognition, compensation, and prevention of SD [29] must be a long lasting task not only for the Chinese doctors but for the government. At least, it is a good sample that the Japanese government passed the “Act on Promotion of Preventive Measures against Karoshi and Other Overwork-Related Health Disorders” [30]. Regarding the updated Physician’s Pledge, the clause “I will attend to my own health” is of paramount importance, so as to provide care of the highest standard for better public health literacy. This urgent strategy, perhaps a sentiment that Hippocrates of Cos would have earnestly countenanced, requires self-alerting consciousness for overloaded medical staff.
In this descriptive study, we have not got the accurate data on the average level doctors due to the limitation of the candidate data of doctors’ health in China, which we are eager to know. A study of prospective or retrospective case-control study by the Chinese Medical Association is required to further disclose age-sex-specific sudden death and life expectancy in Chinese doctors in the near future. Also, there remains lack of the accurate data of sudden death in other occupants in China. It is valuable to carry out the similar studies to further elucidate the sudden death rate of age- and sex matched general population of China. We think this study may deepen the understanding of sudden death of Chinese doctors due to their specific social status in the public health.
In summary, this retrospective study supplied the first evidence of signs of SD. It is urgent to relieve clinical workload and strengthen protection (integration of the establishment of medical labor law, consummation of the hierarchical medical system, optimization of promotion and development of the doctor-patient relationship) against the overload of Chinese medical staff beyond the forthcoming emergency rescue for SD.
The authors have no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper
We acknowledge support from the Medical Research Funding of PLA (ASW14C003) and the Project Program of the Laboratory of Trauma, Burn and Combined Injury, Third Military Medical University (SKLZZ2016). It is historic to commemorate the establishment of The Chinese Doctor’s Day in China on August 19, 2018.

![]()

 |
|
|
 |
|
Figure 1: Occupational status analysis for victims among Chinese medical staff from 2008 to 2018 |
 |
|
Figure 2:Age and gender characteristics for victims among Chinese medical staff from 2008 to 2018 |
 |
|
Figure 3: Regional distribution of karoshi among Chinese medical staff from 2008 to 2018 |
 |
|
Figure 4: Time distribution characteristics of karoshi among Chinese medical staff from 2008 to 2018 (A) Year distribution of victims; (B) Quarter distribution of victims; (C) Month distribution of victims; (D) A period of ten days’ distribution of victims. * P < 0.05, ** P < 0.01 v.s. the control group (2008-2012, quarter1 and 2) |




































