Open Access
Research Article
Max Screen >>
ISSN: 2639-9253
Copyright: © 2018 Nepomuceno-Junior BRV. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Introdution: The sedestation is defined as an act of sitting is a useful therapy for physiotherapy, have reported pulmonary effects ranging from increased lung compliance to improvement in oxygenation. There is lack of this study as a single therapy in critically ill patients, showing still not well defined.
Materials and Methods: This was a descriptive, retrospective study of 337 patients admitted to the study unit period, who underwent treatment at some point of admission. It was validated in the sedestation chair and pending lower limbs. Described demographic variables, the characteristic of sedestation and adverse effects.
Results: The mean age was 61.0 ± 18.2 years, with cardiac disorders (24.9%) being the most common cause of admission. Of the 459 patients tested, 337 sedestation underwent therapy during hospitalization. The average of days that patients in the ICU was evidenced sedestraram a total of 3.7 ± 2.3 days
Conclusion: We observed that sedestation can be used as a routine of conduct under intensive care.
Keywords: Sedestation; Early Mobilization; UCI, Physiotherapy
Positioning therapy aims at organizing the body with better biomechanical alignment, in order to prevent deformities and favor the increase of diaphragmatic torque [1,2]. Currently many studies confirm that changing the body position has direct impact on the respiratory system. The perfusion of the lung parenchyma is privileged to regions dependent on the severity and from this it becomes apparent that the ventilation perfusion (V/Q) is likely to change position against the individual adote [3-5]. Physiotherapy employs therapeutic positioning as a tool for the maintenance of lung function. Increase residual functional capacity and favor lung expansion and bronchial hygiene [1].
The sedestation, defined as the act of sitting, is a useful position which provides better perfusion of the bases, where the pulmonary vasculature is more abundant favoring facilitated diffusion. The ventilation of the alveoli of the base, inside the seated posture is beneficial in increasing the functional residual capacity by 30%, improving the ventilation in the most vulnerable segment pulmonary hypoventilation atelectasis and consequent [5,6].
The diaphragm driving muscle of inspiration, is responsible for about 70% of respiratory muscle work. Its dome shape and their points of insertion and fixation favor the expansion of the chest on the abdominal cavity. lung hyperinflation conditions, such as chronic obstructive pulmonary disease (COPD), changes in content as abdominal ascites, the length change curve - diaphragm tension, may cause dyspnea and increased work of breathing (WOR). In sedestration the diaphragm is vertical, with its fibers in a favorable position for a powerful contraction, thus reducing energy expenditure with breathing [7-12].
Due to lack of studies on the subject, which causes empiricism to perform the sedestation, and no actual delimitation of the population to benefit from such behavior, the present study was intended to describe the profile of the patients who undergo this intervention, and link this therapy the occurrence of adverse effects. The findings are predisposed to encourage further work to seek to define criteria for sedestation patients in ICU, and guide the community therapy for clinical, demographic and functional to carry out this behavior in order to get significant evidence, so that such intervention is encouraged and made possible successfully.
A descriptive, retrospective study found that the clinical and epidemiological profile of hospitalized patients in the general ICU of a private hospital in the city of Salvador, BA was carried out; which even has a general ICU, comprising 20 beds, serving patients from the emergency ward and the operating room of the hospital. The study included all the patients admitted from July to December 2009, of both sexes, which sedestraram during the ICU stay, either in bed with lower limbs (LL) pending or chair; and excluded those whose data recorded in medical records were inconsistent. Secondary data were used, obtained from electronic medical records and indicators of the physiotherapy service of the patients in question. The data collection period covered the months of january to march 2009.
The variables investigated were: gender, age, type of the sitting position (bed or chair), the first day after admission to the sitting position, number of days of completion of the sitting position during relocation of the patient; Adverse effects during sitting position (drop in blood pressure >20%; arrhythmia, desaturation >10%; pneumothorax, psychomotor agitation, loss of devices; falceio LL); airway during sitting position of the individual (or physiological artificial airway via endotracheal tube - or tracheostomy TOT - TQT); length of stay in ICU days; group of diseases affected on admission, the mean residence time in days Mechanical ventilation and ICU outcome (discharge or death) [13].
Sedestation was considered the act of sitting or being seated in both chair with therapist assistance or crane assistance, such as the bedside, using backrest and footrest for comfort and stability. The reason for not sedestation was also evaluated, being considered as the reason the following conditions: no therapeutic indication; hemodynamic instability; psychomotor agitation; patient refusal; ache; presence of devices which impede the conduct. To perform the sedestation were not considered filed indication criteria, this decision being based on clinical decision-duty physiotherapist.
To create the database, we used Excel XP software and the analysis there of in SPSS v 21.0. The data were presented descriptively. Continuous variables were analyzed for measures of central tendency (mean and median) and dispersion (standard deviation) and categorical variables such as ratio.
The research project was approved by the Research Ethics Committee Metropolitan Union for Education and Culture (UNIME), in accordance with Resolution 196/96 of the National Council for Research Ethics. The participating hospital issued consent term to the research.
In the period defined for the study they were admitted 587 patients in the Hospital ICU. Of these, 128 were excluded from the pre - analysis, due to stay in the unit for less than 48 hours. The relative frequency of sedestation in unit in question was 57.4%.
Of the 459 patients tested, 337 sedestation underwent therapy during hospitalization (Figure 1). The mean age was 61.0 ± 18.2 years, with a slight predominance of males in 51.6% and the average stay of patients in the unit was 6.5 ± 1.5 days. The distribution of the reason for admission to the ICU showed that 24.9% of patients sedestraram, have entered the unit by heart disease, followed by 17.9% and 15.2% surgical involvement by neurological disorders.
Regarding day of hospitalization the patient sedestrou, it has shown that achieving this occurred mainly on the 2nd day of admission totaling 48.1% (162) patients, followed by 17.8% (60) who underwent sedestation in the first 24 hours of hospitalization. The average of days that patients in the ICU was evidenced sedestraram a total of 3.7 ± 2.3 days (Table 1).
The sample of patients who underwent sedestation, 26.7% required mechanical ventilation, with mean duration of VM 4.5 ± 1.5 days. Obtaining on the discrimination of air used during sitting position was evident that the vast majority, 89.6% (319), sedestraram under physiological VA, followed by 6.2% who were under use of the endotracheal tube. Of the patients who underwent the use of the VM, 86% (77), started the weaning of the prosthesis, of which 77.9% of these, evolved successfully in the final resumption of ventilatory autonomy (Table 2).
The present study is the first to describe the patients exposed to sedestation profile, not being found in the literature to carry out other work only with such behavior study therapy. Stiller et al. studies on security aspects for the mobilization of critically ill patients, systematically back criteria for safe indication of mobilização [16]. Such criteria have in recent years reported in articles and consensus. However there is a lack in the definition of clinical and functional criteria clearly defined to indicate this therapy. The present work, sees to trace the profile of patients with greater frequency sedestram, it being possible thereby to perform flags describing grounded.
Gender discrimination of patients who underwent sedestation demonstrated approximate ratio of 1: 1 between them. Dean et al. identified more often male (5: 1) in patients with stroke who perform early sedestation such data however appear to have direct influence of neurological pathology estuda6. Does not apply to this study which has population of multiple pathologies.
Zafiropoulos et al. andm study of mechanically ventilated patients after abdominal surgery, observed reduction in respiratory rate and minute volume when in sedestation for a period of 20 minutes, compared with supino for 10 minutes. Corroborating the beneficial conditions sedestation, Behrakis et al. analyzing lung compliance in 10 healthy young adults in different positions: supine decubitus and lateral sedestation, found decrease of this marker in the horizontal position, indeed associated with increased blood flow to the lung and the closure of small vias [10,11].
Gravity during sedestation acts on most of the major joints and bone tissue, providing respectively sensitive and proprioceptive stimuli critical to body spatial organization; and the remodeling of bone matrix. The stimulus generated perpendicular to the bone and articular afferents that generate autonomously, will generate muscle readiness, translated for maintaining the basic muscle tone. The indirect effect of sedestation and gravitational stress are also distributed on the cardio-vascular regulation for adequate perfusion of vital organs, as well as the gastro-intestinal level by increasing the peristalsis [12-14].
With respect to the reason for admission to the ICU, it was identified that the most frequent cause of hospitalization was cardiological pathology (25%), this result is related to the economical use of PEEP fact commonly described in studies in patients using invasive mechanical ventilation with the working Frazeir et al which discloses a 21% incidence of acute myocardial infarction (AMI) VM and claims its use can be detrimental to cardíaca function optimization [15]. In the study by Mehta et al., the use of positive pressure given in the form of NIPPV showed a high incidence of re-infarction, especially in patients exposed to bilevel mode [16]. By contrast the sedestation is described by Sharp et al. sedestation position as the stems and prone gain compliance in patients with congestive heart failure, similar to the use of PEEP [4]. The second and third group are prevalence and neurological surgical patients, which shows clear recommendation employing such a conduit in acute condition.
The most frequent form of sedestation in this study was chair, where 74.1% of patients were on sedestation armchair, 41.8% exclusively armchair has found such relation with the presence and in the unit crane arm with appropriate arms and flexible restraints. Enabling the transfer and safe maintenance of this positioning, converging to low rate of adverse effects on the unit. The physiological airway higher frequency was sterile, followed by orotracheal tube. The sedestation in patients VM is trend and reported in several studies, recommended in Task Force of the European Society of Medicine intensiva [1]. It was reported the occurrence of accidental extubation during sedestation.
Scweickert et al. [17]. in a randomized clinical trial showed early mobilization with intervention earliness of the date of first sedestation in ventilated patients, with results of 3.1 days to go to the chair in the intervention group and 6.2 days in the control group (p <0.0001). We found sedestation the first 2.6 days worth noting that only 26.7% of the current population VM used compared to 100% of the population of those authors. Another author states that in their study withdrawal of the first bed was 11.3 days in the control group and 5.0 days in the group intervention [18]. However, it is here the observation that in our unit was not applied in the study of time a mobilization protocol.
Bailey et al. suggests that early mobilization applies from the moment you initiate the 215 stabilization of acute leading to UCI [19]. Already Mundy et al. sedestation ambulation and applied for at least 20 minutes during the first 24 hours internamento [20]. In our study was more sedestation frenquente on the 2nd day (48.1%), followed by day 1 (17.8%) of admission, showing that most of our population was exposed to sedestation within the first 24 hours of permanence the unit.
Morris et al. in a randomized clinical trial in patients with respiratory insufficiency, proposes mobilization protocol defining that these would be subject to conscious patients sedestation [18]. In the present study we observed that consciousness was not a factor against - indicative of this therapy. This is attributed by the fact that this conduct have ventilation benefits useful to sedated and comatose patients, to make safe therapy in these patients, cranes are used to transfer pads and devices to stabilize proper biomechanical position.
The incidence of mechanical ventilation in patients undergoing sedestation was 26.7% from 77 (85.5%) weaning started, with 24.6% failure rate, the failure rate in the general population of the unit was 27, 9%, such are contained in the index reported by Brochard et al., which reported a randomized trial, comparing weaning methods, failure rates between 08% and 39%. Boles et al. demonstrated the failure rate among different populations of 26% and 61% [21,22].
The overall mortality rate of patients who underwent sedestation was 6.8% lower than the rate of overall mortality unit that was, in the same period of 9.2%. Due to the inconsistency of the data records, can not be calculated scores prognosis of gravity to determine that this therapy had a direct effect in reducing mortality of patients. However, in Soares et al study conducted in the same unit, it demonstrated that early mobilization, including sedestation, showed a strong tendency to reduce mortality in patients who were discontinued from VM [23].
It is aimed to limitation of our study the fact of being retrospective and secondary records and physical therapy indicator data which limited the analysis of variables thought to be important in the study of the project. It is advantage of the fact sedestation be applied to routine in the unit, have trained staff and adequate furniture for such therapy. Such conduct is easily applied and low cost using available devices commonly in the UCI's [23,24 25].
In conclusion, we observed that sedestation can be used as a routine of conduct under intensive care. Mainly applied in cardiac, and neurological surgery patients, which greatly benefit from pulmonary effects such stimulation and motor behavior. The act of sitting can be used early on, most often in the first three days and fashion on the second day. Patients with the most diverse airways should be exposed to sedestation. Being the most limiting factors of the application of this therapy to the lack of therapeutic indication in the judgment of the physiotherapist, the release of the on duty doctor or assistant and hemodynamic instability.

![]()

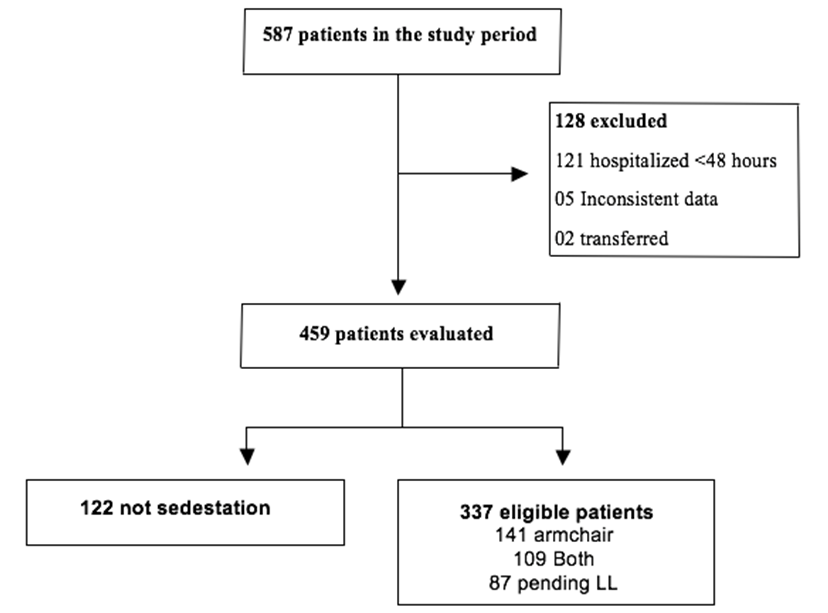 |
| Figure 1: Flowchart of patients in the study period |
|
n(%) |
Mean (SD) |
||||||||
Age, years |
|
61.0 (18.2) |
||||||||
Sex, Men |
174 (51.6) |
|
||||||||
Reason for admission |
|
|
||||||||
Cardiology |
108(25.0) |
|
||||||||
Pneumology |
42 (9.7) |
|
||||||||
Neurology |
66 (15.2) |
|
||||||||
Surgical |
77 (17.8) |
|
||||||||
Vascular / Angiology |
14 (3.2) |
|
||||||||
Medical clinic |
43 (9.9) |
|
||||||||
Nephrology / Urology |
27 (6.2) |
|
||||||||
Gastroenterology |
35 (8.1) |
|
||||||||
Ortho-trauma |
10 (2.3) |
|
||||||||
Oncology |
11 (2.5) |
|
||||||||
Patients sedestation |
337 (57.4) |
|
||||||||
Armchair |
141 (41.8) |
|
||||||||
Pending lower limbs |
87 (25.8) |
|
||||||||
Both |
109 (32.4) |
|
||||||||
Airway the sedestation |
|
|
||||||||
Physiologic |
319 (89.6) |
|
||||||||
Endotracheal tube |
22 (6.2) |
|
||||||||
Tracheostomy |
15 (4.2) |
|
||||||||
Day of the first sedestation |
|
|
||||||||
1st day |
60 (17.8) |
|
||||||||
Day 2 |
162 (48.1) |
|
||||||||
Day 3 |
60 (17.8) |
|
||||||||
Day 4 |
25 (7.4) |
|
||||||||
> Day 5 |
30 (8.9) |
|
||||||||
Table 1: Distribution of demographic and clinical characteristics of patients. |
||||||||||
|
n(%) |
Mean (SD) |
||||||||
Hospital stay |
|
6.5 (1.5) |
||||||||
MV time |
|
4.5 (1.1) |
||||||||
Failure of weaning |
23 (26.0) |
|
||||||||
Outcome |
|
|
||||||||
Discharge from hospital |
314 (93.2) |
|
||||||||
Death |
23 (6.8) |
|
||||||||
Adverse effects* |
9 (2.67) |
|
||||||||
Loss devices |
3 (0.89) |
|
||||||||
Fall to your kneese |
3 (0.89) |
|
||||||||
Reduction in blood pressure> 20% |
2 (0.59) |
|
||||||||
Psychomotor agitation |
1 (0.29) |
|
||||||||
*337 intervention in observed |
||||||||||




































