Open Access
Research Article
Max Screen >>
ISSN: 2394-6520
Copyright: © 2021 Ariff S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Temozolomide is an orally administered chemotherapeutic drug used concurrently with radiation for the treatment of newly diagnosed glioblastoma. Although the addition of Temozolomide has shown to improve overall survival, it is commonly associated with haematological complications. Eltrombopag is an oral thrombopoietin (TPO) receptor agonist that is also used off-label for temozolomide-induced aplastic anaemia.
We report a case of severe prolonged thrombocytopenia in a patient with Glioblastoma Multiforme on Temozolomide. She had a significant drop in platelets from 275 to 53 with pancytopenia. Her thrombocytopenia persisted with platelet nadir of 4 × 109/L for several weeks even after stopping Temozolomide. Haemolytic screening and autoimmune screening were negative. Granulocyte colony-stimulating factor (GCSF) and prednisone along with Human Leukocyte Antigen (HLA) matched platelets were used for support during this period. She required a prolonged hospital stay involving extended packed red cell and platelet transfusion support. There was a slight improvement in white cell and neutrophil counts, eight weeks post-cessation of Temozolomide. Bone marrow aspiration showed markedly hypocellular bone marrow aspirate suggestive of aplastic anaemia or hypoplastic Myelodysplastic Syndrome (MDS). Eltrombopag 50mg daily was commenced, which was tolerated well. There was a significant improvement in the thrombocytopenia within a week of initiating eltrombopag. Platelet transfusions and regular GCSF were stopped as all the parameters continued to show improvement. The platelet transfusion requirement decreased to weekly within a week of starting eltrombopag.
Eltrombopag facilitated a rapid and sustained recovery of platelet count. Our literature review suggests some evidence for the use of thrombopoietin receptor agonists in patients with chemotherapy-related refractory thrombocytopenia. But high-quality safety and efficacy data is limited while waiting for the results of randomised control trials.
Keywords: Oncology; Haematology; Chemotherapy; Thrombocytopenia
List of abbreviations: AE: Adverse Events; ANA: Anti-Nuclear Antibody; ATRX: Alph Thalassemia/Mental Retardation Syndrome X-Linked; CCRT: Concurrent Chemoradiotherapy Group; Cf: Compared To; CIT: Chemotherapy-Induced Thrombocytopenia; COJEC: Cisplatin, Vincristine, Carboplatin, Etoposide, Cyclophosphamide; CTCAE: Common Terminology Criteria For Adverse Events; CVAD: Cyclophosphamide, Vincristine, Adriamycin (Doxorubicin), Dexamethasone; EGFR: Epidermal Growth Factor Receptor; GCSF: Granulocyte Colony-Stimulating Factor; HLA: Human Leukocyte Antigen; IDH1: Isocitrate Dehydrogenase 1 Gene; ICE: Ifosfamide, Carboplatin, Etoposide; ITP: Idiopathic Thrombocypenic Purpura; IV Ig: Intravenous Immunoglobulin; MDS: Myelodysplastic Syndrome; NSCLC: Non-Small Cell Lung Carcinoma; PBS: Pharmaceutical Benefits Scheme; PEG-Rhmgdf: Pegylated Recombinant Human Megakaryocyte Growth and Development Factor; Rhtpo: Recombinant Human Thrombopoietin; Rx: Therapy/Treatment; TERT: Telomerase Reverse Transcriptase; TPO: Thrombopoietin; WCC: White Cell Count.
We are reporting the case of a 63-year-old female who developed significant haematological toxicity related to Temozolomide, used as a part of the Stupp protocol for the treatment of Glioblastoma multiforme.
Her initial presentation was in February 2018 with generalised tonic-clonic seizure and expressive dysphasia. MRI-B revealed subacute left parietal infarction; however, glioma could not be entirely excluded. She subsequently re-presented with confusion and seizures in July 2018, and an intracranial lesion was confirmed on repeat MRI brain. She underwent stereotactic left parietal craniotomy and microsurgical excision of the tumour in October 2018. Histopathology confirmed IDH1 wild type diffuse astrocytic glioma, with retained ATRX and had high-level EGFR amplification (IDH1- Isocitrate dehydrogenase 1 gene, ATRX- Alph thalassemia/mental retardation syndrome X-linked, EGFR- Epidermal growth factor receptor). There was a TERT (telomerase reverse transcriptase) promoter mutation, trisomy 7 and monosomy 10. Based on the immuno-profile, the tumour was managed as glioblastoma as recommended by the multidisciplinary team. Her postoperative recovery was uneventful, and she remained asymptomatic. She did not have any other significant past medical history. She was a life-long non-smoker and rarely drank alcohol. Medications before commencing chemoradiotherapy included levetiracetam, targin, atorvastatin, esomeprazole, and citalopram. Levetiracetam was changed to sodium valproate a few weeks before presentation due to intolerance. Baseline blood tests were within normal limits.
The adjuvant chemoradiotherapy as per the Stupp protocol started on 07 January 2019. Temozolomide was given at a dose of 75 mg/m2 daily as standard practice. Initial complications included grade 1 diarrhoea in the first month, which improved with antidiarrheal medication. On 4th February 2019, week 5 of treatment, a significant drop in platelets from 275 to 53 was noted with stable WCC(white cell count) and neutrophil count. Temozolomide was stopped, but pancytopenia continued to worsen with platelets reaching 13 on 07 February. Due to her remote location more than 3 hours away from the closest regional hospital, she was admitted and platelet transfusions were initiated. During admission the thrombocytopenia continued, refractory to regular platelet transfusions. Haemolytic screening and autoimmune screening were negative other than a borderline ANA (Anti-nuclear Antibody) titre of 1:80 with speckled pattern.
She developed easy bruising, dizziness and non-specific visual symptoms but did not have any bleeding. Her fundoscopy was unremarkable, and repeat brain imaging remained unchanged. By 15 February 2019, she also developed neutropenia, and platelet count further decreased to 4, which prompted daily platelet transfusions. GCSF and prednisone 1mg/kg daily were also introduced. We decided to use HLA matched platelets as recommended by the haematology team as HLA antibody was detected suspected due to poor improvement in platelet counts post-transfusion. The pancytopenia continued to remain refractory more than two weeks after stopping Temozolomide, despite the use of HLA matched platelet transfusion, GCSF and blood transfusions. The increment of platelet count post-transfusion was higher after the use of HLA-matched platelets but was still variable. Due to prolonged severe pancytopenia, she was transferred to a tertiary centre as full-time haematology cover was not available locally. She received almost daily platelet transfusions with only minimal and transient improvement in cell counts between 07 March and 21 May.
Sodium valproate was switched to lamotrigine as it can potentially increase serum temozolomide level, which could have contributed to prolonged thrombocytopenia. There was a slight improvement in white cell and neutrophil counts, eight weeks post-cessation of Temozolomide (Figure 1 and 2). Bone marrow aspiration showed markedly hypocellular bone marrow aspirate suggestive of aplastic anaemia or hypoplastic MDS supporting Temozolomide as the cause of the pancytopenia. Eltrombopag 50mg daily was commenced on 21 May 2019 as recommended by the haematology team based on literature review. Eltrombopag was tolerated well with mild fatigue as the only new symptom. There was a significant improvement in the thrombocytopenia within a week of initiating eltrombopag. The frequency of platelet transfusions dropped which made discharge planning possible. By 12 June, platelet transfusions and regular GCSF were stopped as all the cytopenias continued to show improvement. By 18th July pancytopenia had markedly improved, and both GCSF and Eltrombopag were stopped. Figure 1, Figure 2 and Table 2 show the progression of the WCC, neutrophils, platelets and Hb over time. Although the initial platelet count remained in the low normal range, most cytopenias normalised by September 2019. She continues on close observation, and the last MRI brain from January 2020 remains stable
Although there was a clear faster and sustained recovery within a week of commencing eltrombopag, it is difficult to completely exclude the possibility of the inherent marrow recovery coinciding with the start date. The gradual improvement in the platelet count checked post platelet transfusion can be attributed to the use of HLA matched platelets. The better platelet count response post-transfusion is also likely to be related to the streamlining of the process of harvesting from the identified donors allowing the use of fresher platelets which showed better platelet increments. The platelet transfusion requirement decreased to weekly within a week of starting eltrombopag, the threshold for transfusion being a down-trending platelet count of less than 50. Improvement in pancytopenia was also noted after Eltrmobopag was introduced. Of note, the platelet transfusion threshold decision included consideration of logistical factors like the patient’s remote location. Although the application to commence eltrombopag was made earlier in the course of treatment, there was a significant delay in accessing the medication. The main delay was likely due to eltrombopag not being reimbursed under Medicare Pharmaceutical Benefits Scheme (PBS) in Australia for this indication.
Temozolomide is an orally administered second-generation alkylating chemotherapeutic drug that methylates DNA and prevents tumour cell proliferation [1]. Concurrent therapy with radiation followed by monthly Temozolomide is the standard of care in adults with newly diagnosed glioblastoma. Addition of Temozolomide improved overall 2-year survival from 10.9% to 27.2% as compared to radiotherapy alone. In Stupp protocol, Temozolomide is given at a dose of 75mg/m2 from day 1 to 42 with radiation. After completion of chemoradiotherapy, it is prescribed at a dose of 150 mg/m2 followed by 200mg/m2 depending on tolerance from day 1 to 5, every 28 days [1].
Temozolomide is commonly associated with haematological complications; 55% grade 3 or 4 lymphopenia, 4-19% thrombocytopenia, 8-14% neutropenia and 11% leukopenia [2]. Stupp et al. reported grade 3-4 leukopenia of 7% (2% in concurrent chemoradiotherapy group-CCRT, 5% in the adjuvant group). The rate of grade 3-4 thrombocytopenia was 3% in CCRT group compared to 11% in the adjuvant group with 8% overall discontinuation rate due to toxicities [2]. Other studies have also reported up to 39% overall haematological side effects [2]. In the adjuvant setting, treatment couldn’t be completed in 54% of cases, with a 20% discontinuation rate in concomitant chemoradiotherapy group. Neutropenia (8%) was more common during the CCRT phase compared to the adjuvant phase (3%) [2]. Leukopenia (47.7%), and neutropenia (34.1%) were the most common adverse events as reported in another publication by Kesari et al. [3].
Drug-induced thrombocytopenia is usually immune-mediated. The transfused platelets are also vulnerable to this immune-mediated destruction, which can decrease their lifespan. Platelets express ABO antigens on their surface, as well as HLA class I antigens [4-18]. Studies have demonstrated that the administration of HLA-matched platelets improved both platelet recovery and survival. Furthermore, the degree of match can predict the success of post-transfusion platelet count increments. Platelets survive on an average of 10 days but can vary widely from 15 to 211 hours [19-23]. Hence, there is a need for frequent platelet transfusions, and the incremental response and the duration of survival of platelets can be variable requiring regular monitoring.
Since the discovery of thrombopoietin in 1994, recombinant thrombopoietin molecules like Recombinant human thrombopoietin (rhTPO), and pegylated recombinant human megakaryocyte growth and development factor (PEG-rhMGDF) were developed. Further development was stopped due to concerns over neutralising antibody formation. However, the thrombopoietin receptor agonists were noted to have less risk of antibody formation.
Eltrombopag is oral non-peptide thrombopoietin (TPO) receptor agonist that has been shown to increase the platelet count in both healthy individuals and thrombocytopenic patients with ITP, hepatitis C, or aplastic anaemia. Eltrombopag has also been used along with GCSF for temozolomide-induced aplastic anaemia with a haematological response [4].
There are also reports of the use of other thrombopoietin receptor agonists like romiplostim. There may have been concerns regarding tumour growth stimulation with the use of thrombopoietin agonists. But it is considered safe from this perspective, as studies have shown solid tumours do not possess functional thrombopoietin receptors [21-28]. Hence, these agents have been used in patients with chemotherapy-related refractory thrombocytopenia which, as a result, allowed the safe continuation of chemotherapy [5].
We conducted a literature search for all the reports and studies reporting the use of thrombopoietin agonists in the setting of chemotherapy-induced thrombocytopenia till 20 July 2020 in MEDLINE, EMBASE, Google Scholar and Pubmed. The reported cases and studies are summarised in Table 1 and 2.
The PLATUM trial used Romiplostim in patients who developed grade 3 or 4 thrombocytopenia related to Temozolomide during the chemoradiotherapy for newly diagnosed glioblastoma [15]. Out of 20 patients enrolled, 12 (60%) were able to complete the six cycles of maintenance Temozolomide and four patients discontinued due to progression or unrelated adverse events. 2 (10%) patients did not respond to Romiplostim. Dardis et al. reviewed 28 patients with chemotherapy-induced thrombocytopenia while receiving treatment for glial tumours (glioblastoma, astrocytoma, oligodendroglioma). Either eltrombopag or romiplostim was started at the discretion of the treating physician but typically when platelets count had fallen below 100 X 10 9/L. 95% of patients were able to recommence chemotherapy and continue treatment. The patient who did not respond had previously received chemotherapy for leukaemia during childhood. There was one sudden unexpected death suspected to be pulmonary embolism, although no autopsy was performed [6].
Al-Samkari et al. recently published a study which retrospectively evaluated 170 patients with CIT who were treated with Romiplostim [17]. 150 patients had solid tumours, predominantly gastrointestinal malignancies. 71% of patients achieved a Romiplostim response which was defined as the achievement of platelet count ≥ 75 X 109/L and ≥30 x 109/L above baseline. Furthermore, 79% avoided dose reductions or delays and 89% avoided platelet transfusions. 10% response rate was seen in patients with non-myeloid haematological malignancy with bone marrow involvement. Seven patients developed venous thromboembolism (VTE) without associated thrombocytosis, and no arterial thromboembolic events occurred.
In 2016, Iuliano published results from a study of 22 patients, at high risk of chemotherapy-induced thrombocytopenia (CIT) who received low dose eltrombopag as prophylaxis. CIT was prevented in 21 out of 22 patients in this study [7]. Soff et al. also reported a phase II, open-label trial of romiplostim in solid tumour patients with at least four weeks of thrombocytopenia (100 X 109/L), despite reduction or delay in chemotherapy [8a,8b]. Romiplostim effectively reversed CIT, allowing for resumption and maintenance of cancer-directed therapy in the majority of patients [8]. Natale et al. [13] and Frey et al. [16] reported two separate randomised placebo-controlled phase II trials testing Romiplostim in treatment of CIT in NSCLC and Eltrombopag in the prophylactic use in patients being treated for AML respectively. Both studies did not demonstrate beneficial impact on platelet count related efficacy endpoints. A Cochrane systemic review looked at the current evidence for the use of TPO agonist in chemotherapy-induced thrombocytopenia and found limited quality evidence [16].
Thrombopoietin receptor agonists can be associated with venous thrombosis and the induction of marrow fibrosis [24]. Also, there have been concerns that due to the promotion of hematopoietic stem cells, it might also promote growth or survival of malignant cells. These have limited the widespread adoption of the thrombopoietin agonists in cancer patients receiving chemotherapy. Although Eltrombopag is more convenient due to its oral form, there is no study comparing it with Romiplostim. However, from our review, the trials studying romiplostim reported less thrombotic events and hepatotoxicity. There are multiple randomised phase 3 clinical trials currently in recruiting phase investigating the use of Romiplostim in the setting of chemotherapy-induced thrombocytopenia in NSCLC, ovarian cancer, breast cancer, (NCT03937154) and gastrointestinal cancer (NCT03362177) expected to complete by the end of 2022 or early 2023.
While there have been multiple retrospective and smaller randomised studies looking at the use of thrombopoietin agonists in CIT, the role and indications for their use remains unclear. Thrombocytopenia is one of the commonest dose-limiting side effects with cytotoxic chemotherapy, including Temozolomide. This case report highlights one of the potential specific indications where thrombopoietin agonist can be of great help as rescue therapy in marked prolonged CIT. But the associated risk of the side effects, including hepatotoxicity and thromboembolic complications, should also be taken into account. Although multiple publications support the use of TPO agonists, the consideration of publication bias is also essential. Hence, more quality evidence is required to be able to estimate the benefits compared to the potential toxicities. However, as more clinical trials are underway, we should have more evidence in this area to guide our clinical practice in the near future.
• Temozolomide can cause marked prolonged haematological toxicity which can be very challenging to manage. • Eltrombopag provided a fast and sustained recovery from chemotherapy-induced thrombocytopenia • There was a delay in receiving eltrombopag as it is not listed on the PBS for this indication despite shared pay program from the drug company. • Literature review suggests some evidence for the use of thrombopoietin receptor agonists in patients with CIT but high-quality safety and efficacy data still lacking.

![]()

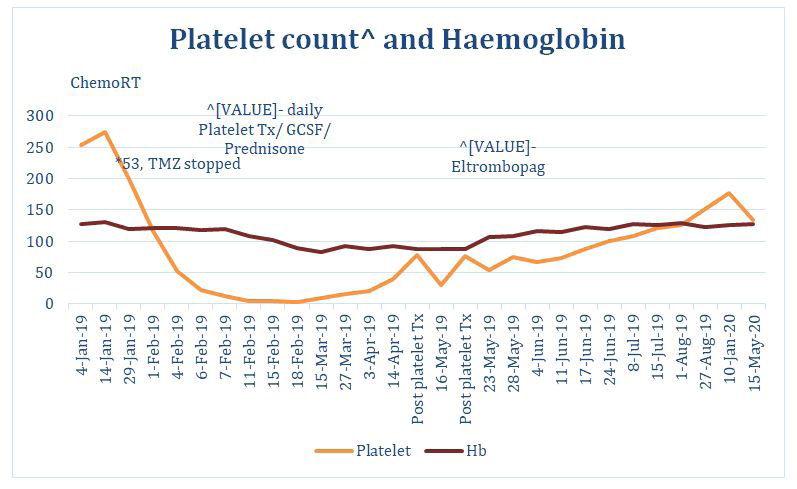 |
Figure 1: Platelets (10*9/L), WCC (10*9/L) and Hb (g/L) levels from 04 January 2019 to 15 May 2020 |
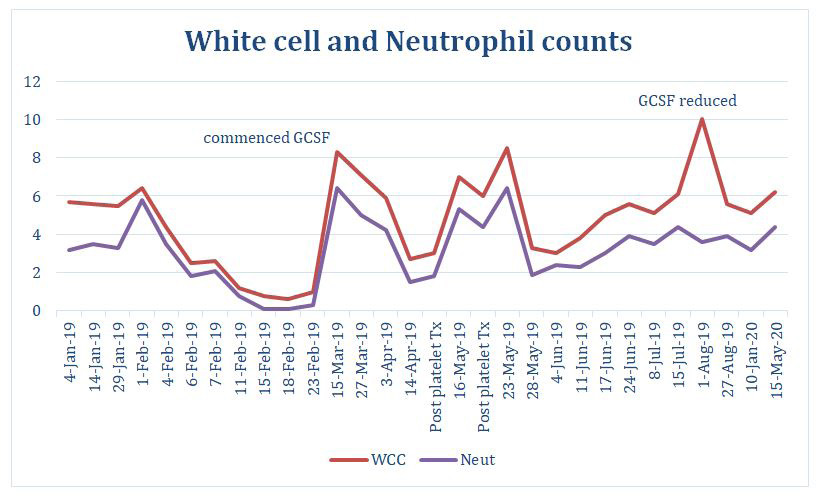 |
Figure 2: WCC (10*9/L) and neutrophil (10*9/L) levels from 04 January 2019 to 15 May 2020 |
Author/year pub- lished/ Drug |
Type of study |
Patient (N) |
Indication for use |
Chemotherapy |
Result |
Al-Samkari et al. [17] 2020 |
Retrospec- tive review |
173 (153 solid tumour- most common GI) |
Treatment of persistent CIT (>3 weeks since last chemotherapy) |
Multiple (most common Platinum, Gemcitabine, Temozolomide, Taxane) |
Clinical benefit in 71% of solid tumor patients with achieving platelet count ≥ 75 X 109/L and at least 30X 109/L higher than baseline |
Le Rhun etal. [15] 2019 Romiplostim |
Phase II single-arm trial |
20 patients with Glioblastoma |
Treatment of CIT after CCRT (Grade 3/4) |
Temozolomide |
12/20 (60%) patients were able to continue treatment (6 cycles) without interruption |
Fassel H etal. [5] 2019 |
Case report in paediat- ric oncology |
2 patients with Neuroblas- toma |
IV Ig and transfusion refractory CIT |
Antineuroblas- toma chemo- therapy (N7 induction, rapid COJEC, ICE) |
Allowed safe and timely continu- ation of chemotherapy without relapse of thrombocytopenia |
Frey et al. [16] 2019 Eltrombopag |
Ran- domised, double blind, Phase II |
148 patients with AML |
Prophylactic use (Day 4 of in- duction, dose escalation if Day 7 platelet count <100x109/L) |
Anthracycline- based |
Eltrombopag did not improve the time to platelet recovery or incidences of grade 3-4 thrombo- cytopenia |
Soff GA et al. [8] 2019 |
Ran- domised phase 2 trial compared to observa- tion |
23 patients with Solid tumours |
Treatment of CIT for at least 4 weeks, despite dose reduction and delay |
Multiple regi- mens |
14 out of 15 (93%) patients randomised to Romiplostim, achieved platelet count correction (≥ 100x10 9/L) within 3 weeks, |
Al-Samkari etal. |
Retrospec- tive analysis |
22 with CIT or pre-existing thrombocytop-nia |
Prophylactic and treatment if Platelet count nadir <100 x10 9/L with or without chemoRx |
Multiple (most common |
18/22 (81%) were able to continue treatment without interruption or dose reduction. |
Iuliano etal. 2018 [25] and 2016 [7] |
Case series |
28 patients, 22 with solid tumours, 6 with DLBC |
Prophylaxis when platelet count |
Platinum-based |
1/28 patient required increased dose of Eltrombopag, all other pa- tients achieved endpoints of avoid- ing Platelet Nadir<50 X 109/L, transfusions, bleeding events, dose reduction or delays. |
Newton etal. [4] 2018 |
Case report |
Patient with GBM |
Treatment of prolonged aplastic anaemia (Platelet Nadir-6) |
Temozolomide |
Benefit noted- hematopoietic recovery at day 131 following first dose of temozolomide |
Dardis, C et al. [6] 2017 |
Retrospec- tive Case Series |
28 patients with Glioma, who developed CIT |
Treatment for CIT (Platelets <100 x10 9/L or physician discretion) |
Temozolomide, bevacizumab, lomustine |
27/ 28 (96%) patients responded, all patients were able to resume chemotherapy and continue for longer time at higher doses than prior to the treatment (median 32 months). |
Author/year pub- lished/ Drug |
Type of study |
Patient (N) |
Indication for use |
Chemotherapy |
Result |
Winer ES et al. [14] 2017 |
Ran- domised placebo controlled Phase 2 |
75 (52 received Rx) |
Treatment for CIT |
Gemcitabine with or without combination with platinum |
shortened the time to platelet count recovery and reduced dose delays/reductions |
Miao, J etal. [ 9] 2016 |
Retrospec- tive Case series |
32 patients, with CIT (59% GI malignancy) |
Treatment for CIT (Mean 68 x10 9/L ) |
Platinum-based |
28 out of 32 (87%) patients re- sponded, and were able to receive 2 or more cycles of chemotherapy without delays or dose reductions for thrombocytopenia, median duration 131.5 days |
Urena LE et al. [28] Romiplostim |
Case series |
15 patients with malignancies (11 non-hematologic) |
Treatment for CIT median baseline platelet count- |
Multiple regi- mens |
87% of patients achieved response, in 11 cases with platelet counts of |
Winer ES et al. [10] 2015 |
Ran- domised placebo controlled phase 1 study |
26 patients planned for gemcitabine monotherapy or combination |
Prophylaxis if platelet count |
Gemcitabine and platinum- based |
14% in Eltrombopag cf. 50% in placebo arm required chemothera- py dose reductions and/or delays Dose not escalated to >100mg/day due to thrombocytosis but no dose limiting toxicity |
Parameswaran, R. et al. [12] 2014 |
Retrospec- tive review |
20 with predominantly solid tumours |
Treatment of protracted CIT (<100× 109/L for at least 6 weeks despite dose delay or reduction) |
Multiple regi- mens |
clinical benefit in 19/20 (95%) patients (platelet count ≥ 100 × 109/L), 15/20 (75%) patients able to resume chemotherapy without recurrence, 14/20 (70%) patients completed more than 2 subse- quent cycles of chemotherapy 3/20 developed DVT |
Chawla et al. [19] 2013 Eltrombopag |
Phase I dose escalation study |
12 with CIT in advanced soft tissue sarcoma |
Treatment for CIT (<75× 109/L with previous chemotherapy) |
doxorubicin and ifosfamide |
Clinical benefit in 11/12 (91%) |
Hayes, et al. [26 ] 2013 |
Pooled Pharma- cokinetic/ pharmaco- dynamic data |
Combined 3 different studies (Kellum [20], Jenkins, Mat- thys 2010) |
Prophylactic (Studies 1 and 2 were in healthy subjects, study 3-Kellum et al.) |
Carboplatin/ paclitaxel |
Eltrombopag stimulated platelet precursor production, propor- tional to plasma Eltrombopag concentration |
Winer, E. S. et al. |
Phase 1 placebo controlled |
26 with solid tumours |
Prophylactic/Treatment (baseline count <300× 109/L, planned for 6 cycles of chemo) |
Gemcitabine with or without Cisplatin or Carboplatin |
Well-tolerated and improved platelet count compared to placebo especially in combination arm (platelet nadir 53 compared to 113) |
Author/year pub- lished/ Drug |
Type of study |
Patient (N) |
Indication for use |
Chemotherapy |
Result |
Kellum et al. [20] 2010 Eltrombopag |
Rand- omized phase 2 study |
183 with advanced solid tumours |
Prophylactic (chemo Naïve, planned for at least 2 cycles of carboplatin at 5-6 AUC) |
First line Carbo- platin/paclitaxel |
Post-chemo nadir platelet counts increased during cycles 1 and |
Vadhan-Raj S etal [27] |
Rand- omized, placebo- controlled, dose and schedule- finding phase I/II study |
50 patients with non-Hodg- kin’s lymphoma |
Prophylactic (patients planned for specific chemo regimen) |
RHyper-CVAD alternating with RArac-MTX |
The platelet nadir was significantly higher and the duration of throm- bocytopenia was shorter, with |
Fanale M et al. (2009) |
open-label dose- and schedule- finding study |
39 patients with lymphoma |
Treatment of CIT (Platelet count <50× 109/L) |
Multiple regi- mens |
No dose-dependent effect on the incidence of serious AEs. One patient with stage IV gastric lym- phoma died following a serious AE of gastrointestinal hemorrhage |
Natale, R et al. [13] 2009 |
Ran- domised placebo controlled Phase 2 |
62 patients with NSCLC (placebo:Romiplostim-12:50) |
Treatment of CIT in previous cycle ( platelet <100× 109/L) |
Gemcitabine and platinum- based |
No evidence of beneficial impact on platelet count related efficacy endpoints. |
CURRENT TRIALS |
NCT03937154 Phase 3 Randomized Placebo-controlled Double-blind Study of Romiplostim for the Treatment of Chemotherapy-induced Thrombocytopenia in Patients Receiving Chemotherapy for Treatment of Non-small Cell Lung Cancer (NSCLC), Ovarian Cancer, or Breast Cancer- estimated completion date: 26 February, 2023 RECITE: A Phase 3 Randomized Placebocontrolled Double-blind Study of Romiplostim for the Treatment of Chemotherapy- induced Thrombocytopenia in Patients Receiving FOLFOX-based Chemotherapy for Treatment of Gastrointestinal or Colorectal Cancer - estimated completion date: 18 December, 2022 |
Date |
WCC |
Neutrophil |
Platelet |
Hb |
Remark |
4 January 2019 |
5.7 |
3.2 |
253 |
127 |
|
7 January 2019 |
Commenced Concurrent ChemoRadiotherapy |
||||
14 January 2019 |
5.6 |
3.5 |
275 |
130 |
Developed grade 1 diarrhoea |
29 January 2019 |
5.5 |
3.3 |
199 |
120 |
|
1 February 2019 |
6.4 |
5.8 |
117 |
121 |
|
2 February 2019 |
|
|
|
|
Stopped dexamethasone due to severe esophagitis |
4 February 2019 |
4.4 |
3.5 |
53 |
121 |
Temozolomide stopped, asymptomatic |
06 February 2019 |
2.5 |
1.8 |
22 |
118 |
|
07 February 2019 |
2.6 |
2.1 |
13 |
120 |
Admission and First Platelet Transfusion |
11 February 2019 |
1.2 |
0.8 |
5 |
108 |
Tx- when Platelet <10 (almost Second daily platelet transfu- sion) |
13 February 2019 |
0.9 |
0.4 |
14 |
104 |
Developed bruising, rashes but no bleeding |
Date |
WCC |
Neutrophil |
Platelet |
Hb |
Remark |
15 February 2019 |
0.8 |
0.1 |
4 |
102 |
Started Prednisone 1 mg/kg/day , daily platelet transfusion, GCSF, with plan to arrange HLA matched platelets, |
18 February 2019 |
0.6 |
0.1 |
3 |
89 |
|
19 February 2019 |
0.8 |
0.1 |
4 |
81 |
No change in Platelet/ Neutrophil count despite stopping temozolomide for 2 weeks |
20 February 2019 |
0.5 |
0.2 |
5 |
76 |
Received last dose of RT ( 29/30 #) prior to transfer to tertiary centre for ongoing haematology input |
23 February 2019 |
1.0 |
0.3 |
2 |
87 |
Platelet Transfusion |
27 February 2019 |
1.9 |
0.7 |
4 |
82 |
|
02 March 2019 |
2.2 |
0.9 |
4 |
89 |
|
07 March 2019 |
2.0 |
0.8 |
9 |
80 |
Post Bone marrow aspiration |
15 March 2019 |
8.3 |
6.4 |
9 |
82 |
Platelet Transfusion |
21 March 2019 |
3.1 |
1.7 |
13 |
90 |
Platelet Transfusion |
27 March 2019 |
7.1 |
5.0 |
15 |
92 |
|
03 April 2019 |
5.9 |
4.2 |
21 |
88 |
|
11 April 2019 |
Application for Eltrombopag |
||||
14 April 2019 |
2.7 |
1.5 |
39 |
93 |
|
Post platelet Tx |
3 |
1.8 |
78 |
88 |
First significant increase in count post HLA matched Platelet Tx |
16 May 2019 |
7 |
5.3 |
30 |
88 |
Platelet Tx |
|
6 |
4.4 |
76 |
88 |
Post Platelet Tx |
21 May 2019 |
Commenced on Eltrombopag 50 mg daily, Platelet transfusion decreased to weekly, Continued GCSF twice weekly |
||||
23 May 2019 |
8.5 |
6.4 |
54 |
107 |
|
28 May 2019 |
3.3 |
1.9 |
74 |
109 |
|
04 June 2019 |
3. |
2.4 |
66 |
116 |
|
11 June 2019 |
3.8 |
2.3 |
73 |
114 |
|
17 June 2019 |
5 |
3 |
87 |
123 |
|
24 June 2019 |
5.6 |
3.9 |
100 |
120 |
|
08 July 2019 |
5.1 |
3.5 |
108 |
128 |
|
15 July 2019 |
6.1 |
4.4 |
121 |
126 |
|
22 July 2019 |
GCSF reduced to weekly dose |
||||
1 August 2019 |
10 |
3.6 |
125 |
129 |
|
27 August 2019 |
5.6 |
3.9 |
151 |
122 |
|
19 September 2019 |
3.8 |
2.2 |
171 |
127 |
|




































