Open Access
Research Article
Max Screen >>
ISSN: 2394-6520
Copyright: © 2021 Ariff S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background: Breast cancer ranks first among the most commonly diagnosed cancers in Kenyan females and globally. Treatment is challenging because it is a heterogeneous disease with several subtypes. There has been a significant change in the treatment of Human Epidermal Growth Factor Receptor 2 (HER2) positive breast cancer subtypes following the introduction and widespread use of HER2 targeted therapies.
Objective: This study evaluated the drug therapy problems and clinical outcomes of trastuzumab-based therapy in patients with Human Epidermal Growth Factor Receptor 2 positive breast cancer
Methods: A cross sectional study design was adopted. It involved 81eligible patients with Human Epidermal Growth Factor Receptor 2 positive breast cancer at Kenyatta National Hospital. Patient records for the period 2014-2019 were retrieved and selected using universal sampling. Analysis of the data was carried out using STATA version 14. Descriptive statistics were used to analyze data.
Results: The mean age of all the patients was 45.98±9.68years, a majority (44, 54.32%) of whom were premenopausal women. Drug interactions, non-adherence to medicines, and adverse drug reactions were the most prevalent drug-related problems. The major causes of non-adherence were patients could not afford the drug product (26, 32.1%) and unavailability of trastuzumab (25, 30.86%). The mean total follow-up period for the entire study population was 24.91±10.44 months. There were 41 (50.62%) patients who demonstrated complete response, 18 (22.22%) progressive disease, 13 (16.05%) partial response while 9 (11.11%) had stable disease.
Conclusion: This study demonstrated a significant positive impact of trastuzumab on the clinical outcomes of patients with HER2 positive early and metastatic breast cancer. Drug therapy problems were common among these patients.
Keywords:Human Epidermal Growth Factor Receptor 2 Breast Cancer; Treatment Outcomes; Drug Therapy Problems
List of abbreviations: ACTH: Doxorubicin, Cyclophosphamide, Paclitaxel, Trastuzumab; ADR: Adverse Drug Reactions; AJCC: American Joint Committee on Cancer; CMF: Cyclophosphamide, Methotrexate, Fluorouracil; CTC: Cancer Treatment Centre; DFS: Disease-Free Survival; EBC: Early Breast Cancer; FISH: Fluorescence In Situ Hybridization; HER2: Human Epidermal Growth Factor Receptor 2; ISH: Immunohistochemistry; KNH: Kenyatta National Hospital; KNH/UON-ERC: Kenyatta National Hospital/ University Of Nairobi-Ethics And Research Committee; LVEF: Left Ventricular Ejection Fraction; MBC: Metastatic Breast Cancer; TAC: Doxorubicin, Cyclophosphamide, Trastuzumab; TCH: Docetaxel, Carboplatin, Trastuzumab; TNM: Extent (Size) Of The Tumor (T), The Spread To Nearby Lymph Nodes (N), The Spread (Metastasis) To Distant Sites (M); WHO: World Health Organization
Breast cancer remains the most common malignancy among females globally and carries a very high mortality. It accounted for 11.6% of the total cancer deaths globally in 2018 [1]. This disease is a significant health problem and a considerable amount of resources are spent in diagnosis, management, surveillance and research of new treatments. The introduction of new therapeutic modalities and early diagnosis has led to significant benefits concerning disease-free survival and overall survival.
Generally, 20-25% of newly diagnosed breast cancers tend to be HER2 positive signifying an aggressive phenotype with a remarkably poor prognosis relative to other breast cancer subtypes [2-4]. Trastuzumab-based therapy has initiated a new milestone in the treatment of HER2 positive breast cancers with proven attractive clinical benefits when used as neoadjuvant or adjuvant therapy for early breast cancer (EBC) and treatment of the metastatic disease [5-9].
However, there is rather scanty real-world information about the clinical outcomes of Trastuzumab-based therapy in the Kenyan population since there are few studies done in Kenya on breast cancer. The cancer multidisciplinary team rely on published data that has mainly been based on western population to make treatment choices. Consequently, patients receive similar treatment intensity despite having different characteristics from the said population. This study will provide information about the clinical outcomes of trastuzumab-based therapy in the Kenyan setting and optimize the use of trastuzumab for the treatment of HER2-positive early and metastatic breast cancers. There is a need therefore to do more research focusing on breast cancer in order to evaluate the clinical outcomes and drug therapy problems of this modality of targeted therapy in Kenya. The findings may help to tailor-make treatment according to our setting and thus improve treatment outcomes.
Kenyatta National Hospital was the study site. The facility is the largest national, teaching and referral hospital in Kenya. It has a cancer treatment center with a radiotherapy unit as well as a chemotherapy administration unit. It also has a well-organized Health Information Department with an updated database.
This was a cross section study concerned with the treatment outcomes of patients with HER2-positive breast cancer. Data was abstracted from patient medical records who were treated with trastuzumab as part of the regimen between 2014 and 2019. Their medical records were retrieved from the health information department.
The sample size was calculated using the single population proportion formula [10]. The corrected sample size with a 15% contingency for incomplete medical records gave a target sample size of 91 medical files. However, only 81 medical records met the inclusion criteria and all of them were included in the study.
The universal sampling method was used to select the patient files. This was because the number of patient records were fewer than what was projected using the formula mentioned in the section immediately above
The study included medical records of a cohort of adult female patients aged 18 years and above. They had been diagnosed with HER2-positive early breast cancer and treated in adjuvant or neoadjuvant setting or for metastatic disease in routine practice. They must have received chemotherapy followed by or combined with trastuzumab. At least six cycles of trastuzumab should have been administered.
Records excluded from the study were for patients with other coexisting malignancies and those with incomplete data.
Effective outcome measures were; tumor response, symptoms resolution, trastuzumab-associated side effects, and overall outcome after therapy (alive or dead). Independent variables were patient and disease characteristics and type of anti-cancer treatment administered. Some possible confounders were concomitant diseases, other types of treatment given, and treatment affordability.
Follow up was estimated from the time of surgical treatment of breast cancer or the start of chemotherapy, whichever occurred first. Disease-free survival was estimated as the period of time from surgical treatment to the first documented disease progression resulting in inoperability, locoregional recurrence (after neoadjuvant therapy), distant metastases, or death from any cause.
Patients who were alive without an event as of the analysis cutoff date were censored at the last date of study follow‐up. The duration of trastuzumab use was calculated from the first day it was used to the last one. One cycle of trastuzumab therapy was defined as an initial loading dose of 8mg/kg or subsequent doses of 6 mg/kg every three weeks.
Tumor response was defined according to the Response Evaluation Criteria in Solid Tumors Group criteria [11]. It was assessed as complete response being tumors that had completely disappeared, partial response being tumors that had shrunk by >30%, stable response being the stable tumors while progressive disease were tumors that had grown by >20%.
Data were obtained from patient records and entered into an abstraction form. This form contained several sections that catered for all the variables of interest. Possible drug interactions were checked using Medscape, Micromedex and Web MB interaction checkers. Du Bois method was used to determine body surface area while Modification of Diet in Renal Disease Study equation was used to Estimate Glomerular Filtration Rate. The American Joint Committee on Cancer (AJCC), TNM staging system was used.
Descriptive data analysis such as frequency, proportion, and percentages were used to summarize categorical variables of patient and tumor characteristics. Continuous variables like the duration of trastuzumab therapy, number of trastuzumab cycles administered and disease-free survival were summarized using mean and standard deviation. Total follow-up period, time to occurrence of relapse and time to treatment failure were also summarized using mean and standard deviation. Breast tumor response to treatment, trastuzumab associated adverse events and drug related problems were analyzed using frequency and percentages.
A total of 81 study patients were included in this study. As shown in Table 1, the mean age of all the study patients was 45.98±9.68 years (range 27-71 years). Most (54, 66.67%) patients were married women and had attained a primary level of education and beyond. Fifty-four (66.67%) were from rural areas and 30(37.04%) were self-employed. Thirty-six (44.44%) patients were overweight.
Forty- four (54.32%) study patients were premenopausal while 61 (75.31%) had a history of contraceptive use (Table 2). Among the patients who were on contraceptives at the time of diagnosis of breast cancer, non-oral hormonal method was the most preferred. Fifty-nine (72.84%) patients had been diagnosed with an early form of breast cancer. The most prevalent comorbidities among these patients were obesity (17, 20.99%) followed by hypertension (15, 18.52%).
The main tumor characteristics are summarized in Tables 3 and 4. Two histopathological types of breast cancer were identified. Ductal carcinoma (78, 96.30%) was predominant. Thirty-two (39.51%) patients had stage III breast cancer at diagnosis while Grade 2 tumors were the most common (36, 44.44%). Overall, HER2 was overexpressed (3+) in 76 (93.83%) patients and HER2 gene was amplified in 5 (6.17%) patients. FISH testing was done for only the IHC equivocal results (2+).
The patients who had estrogen receptor-positive and progesterone receptor-positive breast cancer were 39 (48.15%) and 35 (43.21%), respectively. Thirty-three (40.74%) had a high ki-67(>20%) roliferative index indicating a poor prognostic profile. The majority of patients (69, 85.19%) had recorded a normal Left ventricular ejection fraction at diagnosis.
The majority (61, 75.31%) of the patients had undergone modified radical mastectomy (Table 5). Among nine (11.11%) patients only a biopsy was done while six (7.41%) underwent a breast conserving surgery and three (3.70%) did not undergo any form of surgery. The anthracycline-taxane-based chemotherapy regimen was the most prescribed ( 70, 86.42%) , followed by anthracycline-based (6, 7.41%), others (3, 3.70%) , and taxane-based only chemotherapy in two (2.47%) patients.
ACTH was the most (65,80.25%) commonly prescribed regimen while CMF was the least. Forty-nine (60.49%) patients had undergone radiation to the chest wall and 33 (40.74%) were on hormonal therapy. Sixty (74.07%) received trastuzumab after surgery, 19 (23.46%) as palliative therapy and eight (9.88%) before surgery. Thirty-seven (45.68%) patients received doxorubicin plus cyclophosphamide on day one every three weeks for four cycles, followed by four cycles of paclitaxel concurrent with trastuzumab and then trastuzumab alone for the remaining cycles. Forty-four (54.32%) patients received sequential trastuzumab after completing four cycles of doxorubicin plus cyclophosphamide and four cycles of paclitaxel.
As shown in Table 6, eighty (98.77%) patients were put on first-line chemotherapy agents out of which 65(80.25%) received ACTH. Second-line chemotherapy was prescribed in 14 (17.28%) patients some of whom had also received 1st line treatment. Platinum-based regimens were the most prescribed second line agents. Carboplatin plus docetaxel was the most preferred 2nd line regimen in four (4.94%) patients followed by carboplatin plus paclitaxel regimen and Capecitabine in three (3.70%) patients each. Trastuzumab was prescribed in all patients receiving second-line chemotherapy sequentially or concomitant with chemotherapy. Other medications prescribed were analgesics and antiemetics.
All patients had received at least six cycles of trastuzumab. Thirty-three (40.74%) of them had received a total of six cycles and continuing on treatment as at the last follow up date, four (4.94%) had completed 18 cycles and 3 (3.69%) had received more than 18cycles sequentially despite not having metastatic disease. The mean number of cycles was 8.86±3.99 cycles (range 6-22 cycles). The mean duration of trastuzumab therapy was 9.89±4.23 months (range, 4-24 months). Eleven (13.58%) patients had been on trastuzumab for eight months. Sixteen (19.74%) patients had received trastuzumab for more than one year despite not having metastatic disease. This was as a result of missing one or more cycles of trastuzumab in the course of treatment for various reasons. The mean number of months from the last day of chemotherapy to start of trastuzumab therapy was 2.32±3.133 months (range, 0-14 months). Thirty-seven (45.68%) patients received trastuzumab concurrently with chemotherapy hence there was no interval between the last day of chemotherapy and the start of trastuzumab therapy.
Radiotherapy and/or hormonal therapy were initiated after the patient had completed the full cycles of chemotherapy. Sequencing and timing of radiotherapy coincided with the timing of trastuzumab therapy. At the time, trastuzumab was either being administered as monotherapy following concurrent administration with taxanes after four cycles of anthracyclines plus cyclophosphamide or sequentially after all the cycles of chemotherapy. Some patients had their trastuzumab therapy deferred while undergoing radiotherapy but nine (11.11%) patients had trastuzumab therapy given concurrently with radiation to the chest area. However, none received trastuzumab concurrently with anthracycline-based chemotherapy regimens.
A sizeable number of patients who had completed the full cycles of chemotherapy were delayed starting sequential trastuzumab therapy until they had completed all the radiotherapy sessions.
Categories of drug-related problems are summarized in Table 7. A total of 235 drug-related problems were identified. Drug interactions, non-adherence, and adverse drug reactions (ADRs) were the most prevalent drug-related problems. The need for additional drug therapy accounted for 20 (24.69%) and improper drug selection for nine (11.11%). The most common cause for a dosing problem was the failure to adjust the dose in abnormal laboratory results especially for carboplatin where it was not adjusted according to creatinine clearance. As a result, 6 (7.41%) patients received an overdose while 2 (2.47%) received Sub-therapeutic doses.
A total of 20 patients presented with conditions that required additional drug therapy. Most of them (14, 58.33%) complained of persistent burning pain at the mastectomy site, bone pain and shoulder pain that had remained untreated or required additional therapy for optimal pain control. Cough was not treated in 4 (16.67%) patients. Other conditions that were not managed included nausea and vomiting, dyspnea and hypocalcemia which were experienced by one (4.17%) patient for each.
Non-adherence to medications in this study was defined as missing two or more consecutive cycles of trastuzumab therapy. The major causes were unaffordability of the drug product (26, 32.1%) and unavailability of trastuzumab (25, 30.86%) as shown in Table 8. Inadequate hematological profile was implicated in 11 (13.58%) patients while those awaiting cardiac monitoring or LVEF report had their chemotherapy deferred in 6 (7.41%) cases. Loss to follow up led to non-adherence in 5 (6.17%) patients while those who experienced a decrease in LVEF or were undergoing radiotherapy at the time contributed to non-adherence in 4 (4.94%) each. Poor clinical conditions and unbearable drug side effects were the least common causes for non-adherence.
The most common adverse drug reactions were headache (13, 16.05%), neutropenia (9, 11.11%), nausea and vomiting (8, 9.88%) and pain (8, 9.88%). Also, seven (8.64%) patients developed dyspnea and an equal number had numbness. However, anemia, fatigue, and dizziness were the least prevalent ADRs.
The mean total follow-up period for the entire study population was 24.91±10.44 months (range 10-57 months). Sixty-five (80.25%) patients reported resolution of symptoms. There were 41 (50.62%) complete responses, 13 (16.05%) partial responses, 18 (22.22%) cases of progressive disease while 9 (11.11%) had stable disease as illustrated in Figure 1.
The mean disease-free survival was 19.21±11.2 months (range 6-44 months). Progression of disease was present in 18(22.22%) cases. The mean time to occurrence of relapse was 19.21±11.2 months (range 6-44 months). Treatment failure occurred in 11 (13.58%) patients and the mean time to treatment failure was 5.55±1.44 months (range 3-8 months). Change of regimen was reported in 15 (18.52%) cases and it was mainly due to treatment failure (11, 73.33%) and toxicities (2, 13.33%).
Disease recurrence was observed in 18 study patients. The major type of recurrence was metastases which included distant (13, 68.42%), local (5, 26.32%) and regional spread (1, 5.26%). According to the records, 63 (77.78%) patients were alive, 13 (16.05%) were lost to follow up, 2 (2.47%) had transferred care while 3 (3.70%) were dead due to breast cancer-related maladies. Overall survival after diagnosis and initiation of therapy for the deceased patients were 22 months, 40 months and 84 months respectively.
The treatment of breast cancer is mainly achieved via a combination of several treatment strategies which include surgery, chemotherapy, radiotherapy, and hormonal therapy. The choice of treatment and prognosis is determined by histological type of the disease, stage, and grade of the primary tumor, the menopausal status of patients, hormone receptor status (ER and PR status), HER2 status, patient preferences among others.
Trastuzumab is a humanized monoclonal antibody that targets the extracellular domain of the HER2 receptor. It is an effective therapeutic approach in the management of patients with HER2-positive breast cancers [12]. This drug is the mainstay of systemic treatment of HER2 positive breast cancer in both the early and metastatic settings. In this study, ACTH was the most commonly prescribed regimen while CMF followed by sequential trastuzumab was the least prescribed. Similar studies done across the world show that the standard of care to treat curable HER2-positive breast cancer is to give chemotherapy with the HER2-targeted monoclonal antibody trastuzumab and one commonly used regimen is ACTH. Docetaxel and carboplatin plus trastuzumab (TCH) are also indicated and has less cardiotoxicity and a lower risk of leukemia and myeloid dysplasia compared to ACTH [13,14].
Evidence support the continued use of trastuzumab with 2nd and 3rd line chemotherapeutic agents after disease progression [15-17]. Several large prospective randomized trials across the globe have evaluated adjuvant trastuzumab (post-operative) where its incorporation to chemotherapeutic agents showed significant improvement in DFS and OS [7,18-20]. Trastuzumab was prescribed sequentially and concomitantly with chemotherapy every three weeks. This is contrary to a study done by Perez et al. which recommends incorporation of trastuzumab into a concurrent regimen with taxane as an important standard of care substitute to a sequential regimen because DFS improved when 52 weeks of trastuzumab was added to adjuvant chemotherapy [21].
Cardiac toxicity is one of the most common side effects of trastuzumab treatment, especially in combination with anthracycline agents. It manifests as heart failure, accompanied by a decrease in left ventricular ejection fraction (LVEF) or an asymptomatic decrease in LVEF. In this study trastuzumab therapy was given concurrently with radiation to the chest area in 11.11% of patients. This contrasts other studies which show that increases in the mean dose and low–dose volume of cardiac structures are associated with an increased risk of acute LVEF dysfunction. One of the major toxicities of radiotherapy is cardiotoxicity, hence it can potentiate the cardiotoxic effect of trastuzumab when given concurrently [22,23]. However, none was given concurrently with anthracycline-based chemotherapy regimens due to anticipated cardiac toxicity. This is in agreement with the prior studies which recommend the use of trastuzumab after completing the cycles of anthracycline-based regimen [24].
Moderate drug interaction was the most prevalent drug-related problem followed by non-adherence to medications and this is consistent with a study done by Ting et al. [25]. This can be attributed to the complexity of pharmacological treatment of cancer. There is inherent intrinsic risk of drug-related problems owing to a high risk of comorbidities with negative impact on health outcomes of a patient [26]. The major reasons for non-adherence to therapy were unaffordability and unavailability of the drugs. Trastuzumab is a relatively expensive drug and the cost decreases accessibility in a resource constraint facility like KNH. Lack of insurance cover among patients also contributed to inaccessibility. Cardiotoxicity which is a major concern during trastuzumab therapy was relatively low where only four patients developed a decrease in LVEF. The commonest adverse drug events associated with trastuzumab therapy were headache and neutropenia. Interestingly, there were no previous similar studies done on the prevalence of trastuzumab associated adverse drug events for comparison. Therefore, to the best of our knowledge, this is the first study reporting on the prevalence of trastuzumab related ADRs.
The results confirmed a clear and meaningful trastuzumab benefit on clinical outcomes of patients with HER2-positive EBC and MBC. Patients who reported symptoms resolution were 80.25%. Tumor response was observed in a sizeable number of patients with 50.62% complete response and 16.05% partial response on the last day of follow up. This is fairly comparable to a study that evaluated the activity and safety of two dose levels of trastuzumab as a first-line, single-agent trastuzumab in women with HER2- overexpressing metastatic breast cancer which showed an objective response rate of 34% of patients. In addition, 14% of these patients experienced prolonged stable disease, for a combined clinical benefit rate of 48% [27].
The mean DFS was 19.21±11.2 months. This is in line with several phase III studies done across the world that demonstrated improvement in overall survival and relapse-free survival [6,7,19,21]. A study by Slamon et al. [6] was the first that demonstrated the combination of chemotherapy and trastuzumab as the ideal care for patients with HER2 positive MBC due to its attractive clinical benefits.
However, some patients did not show tumor response where 11.11% showed stable disease while 22.22% had disease progression while on trastuzumab. The major type of recurrence was metastases (68.42%). Resistance to trastuzumab remains a therapeutic challenge despite its remarkable effectiveness on HER2-positive breast cancer. Studies have shown evidence that supports its continued use with 2nd and 3rd line chemotherapy regimens following disease progression on trastuzumab [15,16].
Other agents have been developed targeting the HER2 receptor domain. They include lapatinib, an orally active molecule which is a dual inhibitor of tyrosine kinase and therefore disrupts the HER2 and EGFR pathways. Pertuzumab a recombinant humanized monoclonal antibody targeting the HER 2 extracellular domain blocks its activation. An antibody-drug conjugate called Ado-trastuzumab is also an anti-HER2 agent. It consists of trastuzumab stably conjugated to mertansine (DM1) moiety which has antineoplastic activity. Neratinib is an orally active molecule that irreversibly inhibits tyrosine kinases EGFR and HER2. Afatinib is an orally active irreversible inhibitor targeting EGFR/HER1, HER2 and HER4 (28). However, none of these had been used at KNH as at the time of this study.
This study demonstrated a significant positive impact of trastuzumab on the clinical outcomes of patients with HER2 positive early and metastatic breast cancer. The outcome of treatment was mainly dependent on the stage of the disease. Drug therapy problems were common among these patients.
Trastuzumab should be adopted as the ideal standard of care for patients presenting with HER2-positive breast cancer in KNH and other county referral hospitals in Kenya due to its positive impact on the treatment outcomes of these patients. The drug should be made available to deserving patients at KNH to prevent non adherence due to lack of affordability.
Potential limitations of this study were due to its retrospective design and therefore no recourse for the missing data. The length of follow up could have been relatively short and thus insufficient to draw firm conclusions in terms of overall survival and some late recurrences might possibly have been missed. The sample size was also smaller than expected since only one institution was involved. Despite these limitations, our study had several strengths.
To all the faculty members of the school of Pharmacy University of Nairobi and staff of Kenyatta National Hospital Health Information Department for their unyielding support during this study.
This study was self-funded.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
KC conceptualized the idea, conducted the actual study and the statistical analysis and drafted the manuscript. PK and IW were involved in developing the idea, designing of the study, data analysis, and interpretation as well as manuscript writing. All authors approved the final manuscript for publication.
Permission to carry out this study was granted by the KNH/UON Ethics and research committee (KNH/UON-ERC, Approval reference no. P/180/03/2019). Consent and approval were also granted by KNH administration after registering the study with the KNH research and programs department while formal approval to access patient files was granted by the Head of Department of Medical Records. Information obtained was treated with the utmost confidentiality and only used for the intended purpose. Patients’ names and inpatient or outpatients’ numbers were not recorded but they were serialized using unique study numbers.

![]()

Characteristic |
Frequency n (%) |
Characteristic |
Frequency n (%) |
Age category |
|
Form of employment |
|
20-29 |
3 (3.70%) |
Permanent |
18 (22.22%) |
30-39 |
21 (25.93%) |
Casual |
5 (6.17%) |
40-49 |
31 (38.27%) |
Self-employed |
30 (37.04%) |
50-59 |
17 (20.99%) |
Unemployed |
28 (34.57%) |
60-69 |
7 (8.64%) |
Residence |
|
≥70 |
2 (2.47%) |
Urban |
26 (32.10%) |
Mean ± SD |
45.98±9.68 |
Rural |
54 (66.67%) |
Marital status |
|
Not recorded |
1 (1.23%) |
Single |
14 (17.28%) |
BMI category |
|
Married |
54 (66.67%) |
18.5-24.9 Normal |
27 (33.33%) |
Divorced |
5 (6.17%) |
25-29.9 Overweight |
36 (44.44%) |
Widowed |
8 (9.88%) |
≥30 Obese |
18 (22.22%) |
Level of education |
|
|
|
None |
8 (9.88%) |
|
|
Primary |
25 (30.86%) |
|
|
Secondary |
32 (39.51%) |
|
|
Tertiary |
16 (19.75%) |
|
|
Table 1: Sociodemographic characteristics of study patients (n=81)
Characteristic |
Frequency (n, %) |
History of contraceptive use |
|
Yes |
61 (75.31%) |
No |
20 (24.69%) |
Method of contraception |
|
Combined oral contracep- tives |
8 (9.88%) |
Non-oral hormonal |
12 (14.81%) |
Barrier methods |
7 (8.64%) |
Sterilization |
2 (2.47%) |
None |
51 (62.96%) |
Herbal |
1 (1.23%) |
Menopausal status |
|
Pre-menopausal |
44 (54.32%) |
Post-menopausal |
37 (45.68%) |
Category of breast cancer |
|
Early breast cancer |
59 (72.84%) |
Metastatic breast cancer |
22 (27.16%) |
Table 2: Patient baseline characteristics (n=81)
Characteristic |
Frequency (n, %) |
Characteristic |
Frequency (n, %) |
Histology |
|
Metastasis |
|
Ductal |
78 (96.30%) |
Mx (unknown) |
9 (11.11%) |
Lobular |
3 (3.70%) |
M0 |
51 (62.96%) |
Tumor size |
|
M1 |
21 (25.93%) |
T1 |
4 (4.94%) |
Clinical stage |
|
T2 |
30 (37.04%) |
I |
3 (3.70%) |
T3 |
22 (27.16%) |
II |
16 (19.75%) |
T4 |
12 (14.81%) |
III |
32 (39.51%) |
Tx (Unknown) |
13 (16.05%) |
IV |
22 (27.16) |
Nodal status |
|
Unknown |
8 (9.88%) |
N0 |
11 (13.58%) |
Clinical grade |
|
N1 |
14 (17.28%) |
G1 |
4 (4.94%) |
N2 |
23 (28.40% |
G2 |
36 (44.44%) |
N3 |
10 (28.40%) |
G3 |
32 (39.51%) |
Nx (Unknown) |
23 (28.40%) |
Unknown |
9 (11.11%) |
Table 3: Grading and staging of the breast tumor (n=81)
Characteristics |
Frequency n (%) |
|
HER2 Receptor status |
||
IHC |
(2+) borderline |
5 (6.17%) |
(3+) overexpressed |
76 (93.83%) |
|
FISH |
Amplified(positive) |
5 (6.17%) |
Estrogen receptor status |
|
|
Negative |
42 (56.79%) |
|
Positive |
39 (48.15%) |
|
Progesterone receptor status |
|
|
Negative |
46 (56.79%) |
|
Positive |
35 (43.21%) |
|
Ki67 |
|
|
Low (<10%) |
3 (3.70%) |
|
Borderline (10-20%) |
5 (6.17%) |
|
High (>20%) |
33 (40.74%) |
|
Not recorded |
40 (49.38%) |
|
LVEF |
|
|
Borderline (50-55%) |
3 (3.70%) |
|
Normal (˃55%) |
69 (85.19%) |
|
Not recorded |
9 (11.11%) |
|
Key: IHC = Immunohistochemistry; FISH = Fluorescence in Situ Hybridization; LVEF = Left Ventricular Injection Fraction; SD = Standard Deviation
Table 4: Hormonal characteristics of the breast tumor (n=81)
Type of procedure/ Treatment |
Frequency n (%) |
Type of treatment/ procedure |
Frequency n (%) |
Surgery |
|
Chemotherapy regimens |
|
Breast-Conserving surgery |
6 (7.41%) |
ACTH |
65 (80.25%) |
Total mastectomy |
61 (75.31%) |
TAC |
3 (3.70%) |
Biopsy |
9 (11.11%) |
CMF |
2 (2.47%) |
Unknown |
2 (2.47%) |
Others |
11 (13.58%) |
None |
3 (3.70%) |
Radiotherapy |
49 (60.49%) |
Chemotherapy regimens |
|
Hormonal therapy |
33 (40.74%) |
Anthracycline based |
6 (7.41%) |
Trastuzumab after surgery |
60 (74.07%) |
Taxane based |
2 (2.47%) |
Trastuzumab before surgery |
8 (9.88%) |
Anthracycline and taxane-based |
70 (86.42%) |
Trastuzumab as palliative therapy |
19 (23.46%) |
Others |
3 (3.70%) |
Trastuzumab treatment |
|
|
|
Combined with taxanes |
37 (45.68%) |
|
|
Monotherapy |
44 (54.32%) |
Key: ACTH = Doxorubicin, Cyclophosphamide, Paclitaxel, Trastuzumab; TAC = Doxorubicin, Cyclophosphamide, Trastuzumab; CMF = Cyclophosphamide, Methotrexate, Fluorouracil
Table 5: Management approaches to HER2-positive breast cancer (n=81)
Type of therapy/ Regimen |
Frequency (n, %) |
Type of therapy/ Regimen |
Frequency (n, %) |
1st line chemotherapy |
|
Type of 2nd line drugs used |
|
Yes |
80 (98.77%) |
Capecitabine/trastuzumab |
3 (3.70%) |
No |
1 (1.23%) |
Carboplatin/docetaxel/trastuzumab |
4 (4.94%) |
Type of 1st line regimen used |
|
Carboplatin/gemcitabine/trastuzumab |
1 (1.23%) |
ACTH |
65 (80.25%) |
Carboplatin/paclitaxel/trastuzumab |
3 (3.70%) |
TAC |
3 (3.70%) |
Carboplatin/trastuzumab |
1 (1.23%) |
CMF |
2 (2.47%) |
Cisplatin/gemcitabine/trastuzumab |
2 (2.47%) |
CAF |
3 (3.70%) |
|
|
AC |
4 (4.94%) |
Other medications prescribed |
|
ACH |
4 (4.94%) |
Yes |
62 (76.54%) |
2nd line chemotherapy |
|
No. |
19 (23.46%) |
Yes |
14 (17.28%) |
|
|
No |
67 (82.72%) |
|
|
Table 6: Drug regimens used in the management of HER2-positive breast cancer (n=81)
Type of drug therapy problem |
Frequency (n, %) |
Medication use without indication |
6 (7.41%) |
Improper drug selection |
9 (11.11% |
Need for additional drug therapy |
20 (24.69%) |
Sub-therapeutic dose |
2 (2.47%) |
Overdose |
6 (7.41%) |
Failure to adjust the dose in abnormal laboratory results |
8 (9.88%) |
Drug interaction |
78 (96.30%) |
Non-adherence to medication |
65 (80.25%) |
Adverse drug reaction |
41 (50.62%) |
Table 7: Categories of drug-related problems
Reasons for medication non-adherence |
Frequency (n, %) |
Inadequate hematological profile |
11 (13.58%) |
Poor clinical condition |
1 (1.23%) |
Decrease in LVEF |
4 (4.94%) |
The patient couldn’t afford the drug product |
26 (32.10%) |
Drug unavailability |
25 (30.86%) |
Unbearable drugs side effects |
1 (1.23%) |
Patient felt better |
2 (2.47%) |
The patient lost to follow up |
5 (6.17%) |
Awaiting cardiac monitoring or LVEF report |
6 (7.41%) |
The patient was undergoing radiotherapy |
4 (5.00%) |
Key: LVEF = Left Ventricular Injection Fraction
Table 8: Reasons for non-adherence to trastuzumab therapy (n=65)
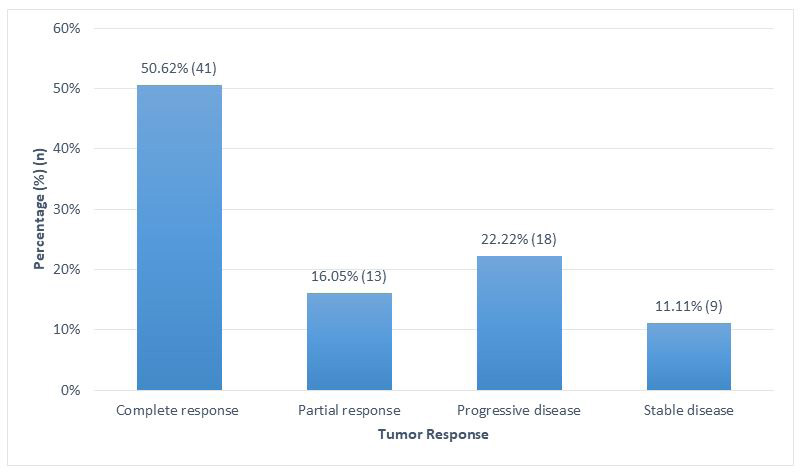 |
Figure 1: Breast tumor response to treatment |




































