Open Access
Research Article
Max Screen >>
ISSN: 2394-6520
Copyright: © 2021 Ariff S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Objective: The aim of this study was to compare and determine the feasibility, surgical outcomes, intraoperative and postoperative complications of the use of the posterior approach technique in the laparoscopic radical hysterectomy (LRH) to the conventional laparoscopic radical hysterectomy in patients with cervical cancer.
Method: From March 2016 to October 2017, we conducted a randomized controlled trial including 50 FIGO stage Ib-IIa cervical cancer participants undergoing LRH from Gynecology Department of Nanjing Maternal and Child Health Care Hospital. All participants were randomly divided into study (23 cases) and control (27 cases) groups. Study group participants underwent posterior approach technique in LRH, while control group participants underwent conventional LRH. Variables such as age, BMI, histological results, FIGO stage, Karnofsky performance status (KPS) score, operating time, intraoperative blood loss, number of dissected lymph nodes, gastrointestinal exhaust time, catheter removal time, abdominal drainage tube removal time, days of hospitalization, complications and their Clavien’s systematic classification were reviewed.
Results: Both groups showed similar patient and tumor characteristics. In surgical outcome analysis, study group showed significantly shorter operating time than Heo YJ et al. reported in the literature (248.96±42.66mins vs 283.0±58.7mins, p=0.03), while t control group showed no significant differences in operating time than Heo YJ et al. reported in the literature (282.22±81.45mins vs 283.0±58.7mins, p=0.97), operating time in study group was with the trend of decrease compared with control group (248.96±42.66mins vs 282.22±81.45mins, p=0.15). Both groups showed significantly lower intraoperative blood loss than than Heo YJ et al. reported in the literature (185.4±193.6ml vs 436.4±201.3ml, p=0.0001; 296.3±201.4ml vs 436.4±201.3ml, p=0.02), study group showed significantly lower intraoperative blood loss than control group (185.42 ±193.64 mL vs 296.30 ±201.40 mL, p=0.04). Both groups showed no significant differences in hospital stay than Heo YJ et al. reported in the literature (16.39 ± 4.45 days vs 19 ±3.73 days, p=0.49; 19.89 ±6.82 days vs 19 ±3.73 days, p=0.59), study group showed significantly shorter hospital stay than control group (16.39 ± 4.45 days vs 19.89 ±6.82 days, p=0.03). Abdominal drainage tube removal time in study group was with the trend of decrease compared with control group (6.35±3.01days vs 8.07±4.41days, p=0.09). There was no significant difference in number of dissected lymph nodes, gastrointestinal exhaust time and catheter removal time between 2 groups. In complications analysis, there were no intraoperative complications in 2 groups. 2 cases of postoperative complications were identified in study group (1 ureteral fistula and 1 urinary retention), while 5 cases of postoperative complications were identified in control group (1 ureteral fistula, 1 pelvic infection, 2 urinary retention and 1 venous thrombosis of the lower extremities). The morbidity rate of postoperative complications in study group was with the trend of decrease compared with control group (8.70% vs 18.52%, p=0.43).There was no significant differences in Clavien’s systematic classification of postoperative complications between 2 groups. All participants had no special discomfort and no abnormality was found in all tests during follow-up.
Conclusion: The use of posterior approach technique in LRH in patients with cervical cancer can significantly reduce intraoperative blood loss, shorten hospital stay, operating time and the morbidity rate of postoperative complications are with the trend of decrease.
Keywords:Cervical Cancer; Laparoscopic Radical Hysterectomy; Side-Injury; Randomized Controlled Trial
Cervical cancer is the fourth most frequent cancer in women [1]. Originally described by Wertheim in the 1890s and subsequently re-popularized by Meigsin the 1950s, abdominal radical hysterectomy (RH) has long been established as a standard treatment for early stage cervical cancer [1]. Although RH represented the standard surgical approach for many years, minimally invasive approaches have been widely adopted in gynecologic oncology over the past few decades [1,2]. Despite the excellent 5-year overall survival rate, the surgical treatment resulted in substantial long-term morbidity, such as lower urinary track dysfunction, sexual dysfunction and colorectal motility disorders [1,2]. Laparoscopic radical hysterectomy (LRH) was introduced to decrease the morbidity of the operative procedure. Numerous retrospective studies have compared laparoscopic and abdominal radical hysterectomy for cervical cancer, and showed that the laparoscopic approach is oncologically safe and associated with fewer postoperative complications and earlier recovery [1-8].
Although LRH has made considerable progress in reducing surgical complications, intraoperative bleeding and perioperative complications are still challenging problems for gynecologic oncologists, among which bleeding from deep uterine vein injury is an important cause. In recent years, we have found that the use of the “posterior approach” technique in LRH for cervical cancer can significantly reduce intraoperative blood loss and shorten hospital stay, now it is reported as follows.
From March 2016 to October 2017, we conducted a prospective randomized controlled trial including 50 cervical cancer participants undergoing LRH from Gynecology Department of Nanjing Maternal and Child Health Care Hospital. All participants were randomly divided into study (23 cases) and control (27 cases) groups. All participants met the inclusion and exclusion criterias and signed written informed consents. All operations were performed by the same group of surgeons who were skilled in performing LRH.
(1) The participant is confirmed cervical cancer by pathological biopsy before the operation. (2) Imaging studies, such as pelvic B-scan ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI), proved that no other metastases were present. (3) FIGO stage was Ia2-IIa. (4) The participant is healthy and can adapt to an extensive operation (has no cardiopulmonary dysfunction and can tolerate the Trendelenburg posture)
(1) FIGO stage was IIb or higher. (2) The participant had major organ dysfunction. (3) The participant had severe coagulation disorders. (4) The participant was combined with other malignant tumors or had infectious diseases that were difficult to control.
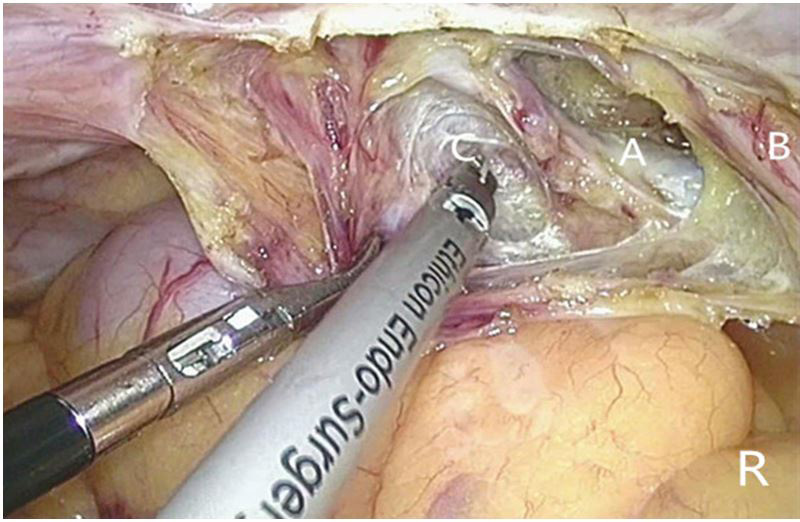
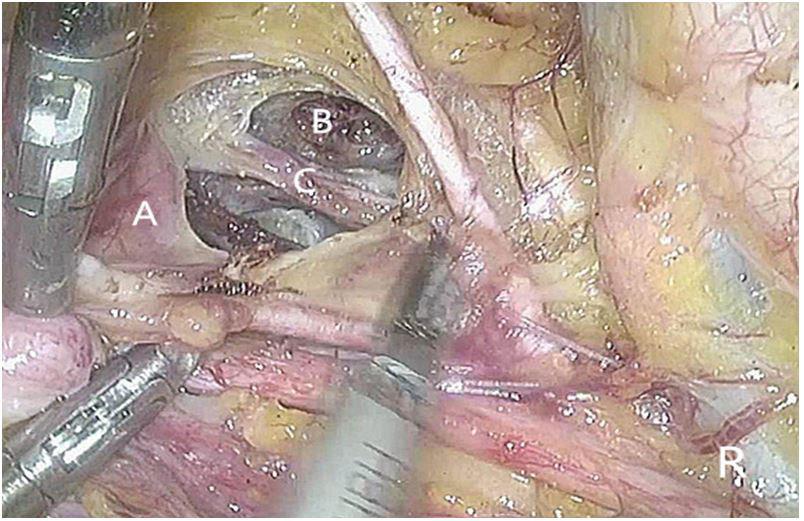
The surgical plan of participants in both groups was “laparoscopic radical hysterectomy + pelvic lymph node resection ± para-abdominal aortic lymph node resection”. The participants in both groups underwent preoperative preparation, anesthesia, disinfection, placing drapes, trocar insertion and abdominopelvic cavity examination according to the routine. Control group participants underwent conventional LRH, while study group participants underwent the posterior approach technique in LRH, and its technical points were as follows: first, we identified one ureter, opened up the ipsilateral retroperitoneum to the beginning of the ipsilateral sacral ligament along the ureter and exposed it (Figure 1). Second, we separated downwards to the Okabayashi gap between the sacral ligament and the ureter, where the hypogastric nerves along the outside of the rectum were exposed clearly (Figure 2). Lastly, we expanded the Okabayashi gap on both sides and separated the loose connective tissue space forward and down to connect with the bladder lateral space, continued separating downwards into the rectum lateral space, where the cervix branch, the forward bladder branches (usually 3 to 4 branches), the main deep uterine veins and sometimes the vaginal branches of the ipsilateral deep uterine vein were exposed clearly in turn from top to bottom (Figure 3). On the opposite side the posterior approach technique was conducted the same way .Thus when the procedure of “opening the ureteral tunnels” was carried out, the ureteral tunnels can be opened only by separating the branches of the ureteral and uterine arteries because the tissues and vessels blow the ureter were fully separated before. When the procedure of “cutting off the uterine main ligaments” was carried out, the parametrial tissues only remained the main deep uterine veins, branches as well as the hypogastric nerve bundles, thus the main deep uterine veins and branches could be cut off in turn and the hypogastric nerve bundles could be reserved.
In this study, the rectum lateral space was defined as: the medial side was composed of the rectum lateral wall and the uterosacral ligament, and the lateral side was composed of the ureter and its mesangium, which was the same as the rectum lateral space proposed by Okabayashi [1]. The bladder lateral space was defined as: the medial side was composed of the bladder column and bladder lateral wall, the lateral side was composed of the umbilical lateral ligament and the bladder subventral fascia below, the cephalic side was composed of the uterine main ligament, the caudal side was composed of the junction of the umbilical lateral ligament and the bladder wall, and the bottom was composed of the levator ani muscle, which was the same as the report of Su yingkuan et al. [2,3].
We used the Statistical Package for the Social Sciences 22.0 (SPSS Inc., Chicago, IL, USA) for statistical analysis. Kolmogorov-Smirnov test was used to verify standard normal distributional assumptions. Student’s t-test and Mann-Whitney U test were used for parametric and non-parametric variables, respectively. Differences between proportions were compared using Fisher’s exact test or Χ2 test. p0.05 was considered to be statistically significant.
This study was approved by the medicine ethics committee of Nanjing Maternal and Child Health Care Hospital (File No. (2016) 17), all participants signed written informed consents for this study.
The participant demographics are shown in Table 1. No significant statistical differences were found with respect to age (p=0.10), BMI (p=0.11), histology (p=0.55), FIGO stage (p=0.39) and Karnofsky performance status (KPS) score (p=0.59) in comparing study group and control group.
As seen in Table 2, variables such as operating time, intraoperative blood loss, number of dissected lymph nodes, gastrointestinal exhaust time, catheter removal time, abdominal drainage tube removal time and days of hospitalization were compared in 2 groups. Study group showed significantly shorter operating time than Heo YJ et al. reported in the literature (248.96±42.66mins vs 283.0±58.7mins, (p=0.03), while control group showed no significant differences in operating time than Heo YJ et al. reported in the literature (282.22±81.45mins vs 283.0±58.7mins, p=0.97), operating time in study group was with the trend of decrease compared with control group (248.96±42.66mins vs 282.22±81.45mins, p=0.15). Both groups showed significantly lower intraoperative blood loss than than Heo YJ et al. reported in the literature (185.4±193.6ml vs 436.4±201.3ml, 0070=0.0001; 296.3±201.4ml vs 436.4±201.3ml, p=0.02), study group showed significantly lower intraoperative blood loss than control group (185.42 ±193.64 mL vs 296.30 ±201.40 mL, p=0.04). Both groups showed no significant differences in days of hospitalization than Heo YJ et al. reported in the literature (16.39 ± 4.45 days vs 19 ±3.73 days, p=0.49; 19.89 ±6.82 days vs 19 ±3.73 days, p=0.59), study group showed significantly shorter hospital stay than control group (16.39 ± 4.45 days vs 19.89 ±6.82 days, p=0.03). Abdominal drainage tube removal time in study group was with the trend of decrease compared with control group (6.35±3.01days vs 8.07±4.41days, p=0.09). There was no significant differences in number of dissected lymph nodes (20.96±7.75 vs 21.93±6.72, p=0.44), gastrointestinal exhaust time (2.65±0.71days vs 2.52±0.80days, p=0.47) and catheter removal time (14.17±3.96days vs 15.04±5.91days, p=0.73) between 2 groups. There was no conversion between 2 groups and no participants withdrew.
Complication data were categorized into intraoperative and postoperative complications (Table 3). There were no intraoperative complications in 2 groups. 2 cases of postoperative complications were identified in study group, one case was ureteral fistula, which was discharged after ureteral stent placement. The stent was removed and the ureteroscopic examination indicated recovery after 3 months. Another case was pelvic infection, which was cured and discharged after treatment with antibiotics and drainage. 5 cases of postoperative complications were identified in control group. 1 case was pelvic infection, which was discharged after treatment with antibiotics and drainage. 2 cases were urinary retention, which were discharged after placement of indwelling urinary catheters. Both cases had normal urination after removal of the catheter within 1 month, review of bladder residual urine B-scan ultrasound indicated recovery. 1 case was ureteral fistula, which was discharged after ureteral stent placement. The stent was removed and the ureteroscopic examination indicated recovery after 3 months. 1 case was venous thrombosis of the lower extremity. Low-molecular-weight heparin was administered by subcutaneous anticoagulation during the hospital stay. Review of deep vein ultrasonography of the lower extremities indicated recovery after 3 months from discharge.
The morbidity rate of postoperative complications in study group was with the trend of decrease compared with control group (8.70% vs 18.52%, p=0.43).There was no significant differences in Clavien’s systematic classification of postoperative complications between 2 groups (p=0.42).
All participants were reviewed once every 3 months at out participant clinics within 6 months after surgery, including: (1) symptoms: urination, bowel habits, and sexual life; (2) full-body and pelvic examination; (3) blood routine, liver and kidney function; (4) tumor marker examination: such as blood SCC and CA125; (5) vaginal cytology and HPV detection; (6) pelvic and abdominal B-scan ultrasonography; (7) CT, MRI, and PET-CT (used when recurrence is suspected); (8) chest radiograph. All participants had no special discomfort and no abnormality was found in all tests.
Intraoperative bleeding can increase operation time, exert unfavorable effects on postoperative recovery and prolong hospital stay. On the one hand, Intraoperative bleeding leads to unclear surgical field of vision, which leads to surgical side injuries easily, thus causing various intraoperative and postoperative complications. On the other hand, the use of the bipolar electrocoagulation,ligasure or other operative energy instruments for hemostasis during operation is also an important cause of surgical side injuries. Heo YJ et al. reported that intraoperative blood loss in LRH was 436.4±201.3ml, the morbility rate of intraoperative and postoperative complications of minimally invasive radical hysterectomy (including LRH and robotic radical hysterectomy) was 1.7%-5.0% and 8.0%-27.0% respectively, the morbility rate of urinary retention was 27.0%-36.0%, days of hospitalization were 19.0±17.5days, and deep uterine vein injury is the main risk [1-4,19].The so-called “radical” in cervical cancer surgery mainly refers to the removal range of the paracervical (or parametrial) and paravaginal tissues, which are mainly composed of the uterine main ligaments. Therefore, RH is mainly the removal of the uterine main ligaments. The uterine main ligaments are surrounded by double fascias, and the “inner core” is located between the bladder and the rectum lateral space, mainly composed of blood vessels and nerves. The blood vessels of uterine main ligaments vary widely, including superior urinary bladder artery, uterine artery, superficial uterine veins, deep uterine veins, and even rectal branch veins [19]. In conventional LRH, opening the ureteral canals and separating downwards the deep uterine veins often results in bleeding because of damage to the complicated bladder branches of deep uterine veins. We used the posterior approach technique to open the retroperitoneum and separate the rectum lateral space first. Since the main deep uterine veins, their larger vein branches and the hypogastric nerve bundles go through in this area and can be identified easily, it is relatively easy and safe to separate the main deep uterine veins and their branches. Thus when the procedure of “opening ureteral tunnels and cutting off uterine main ligaments “ is carried out, because the tissues and vessels blow the ureter have been fully separated before, the bladder branches of the deep uterine veins are easy to be identified, as well as the main deep uterine veins, their branches and the hypogastric nerve bundles have been fully separated before, it is relatively easy and safe to open ureteral tunnels, cut off the uterine main ligaments and reserve hypogastric nerve bundles, which reducing intraoperative bleeding, surgical side injuries and accelerating postoperative recovery [20-22].
This study results indicated that intraoperative blood loss was significantly lower in both groups than Heo YJ et al. reported in the literature mentioned before (185.4±193.6ml vs 436.4±201.3ml, p=0.0001;296.3±201.4ml vs 436.4±201.3ml, p=0.02).The intraoperative blood loss of study group was significantly lower than control group (185.42±193.64ml vs 296.30±201.40ml, p=0.04). Hospital stay of study group was significantly shorter than control group (16.39±4.45days vs 19.89±6.82days, p=0.03). Although there was no significant difference in postoperative complications between 2 groups, the postoperative complications in study group was with the trend of decrease compared with control group (8.70% vs 18.52%, p=0.43). All participants in both groups were followed up for 6 months without postoperative complications. This study results indicated that the use of posterior approach technique in LRH for cervical cancer can significantly reduce intraoperative bleeding and shorten hospital stay, thus accelerate postoperative recovery.
This study also has some limitations. First, the number of cases was relatively small (23 cases in study group, and 27 cases in control group). Second, both the participants and the surgeons came from Gynecology Department of Nanjing Maternal and Child Health Care Hospital, therefore the study was based at a single center, not multi-center. Lastly, the follow-up time was designed to be 6 months, though there were no postoperative complications in both groups during the follow-up period; the long-term oncologic outcomes had remained unknown.
This study results indicate that compared with conventional LRH, the use of the posterior approach technique in LRH can significantly reduce intraoperative blood loss and shorten hospital stay, which is safe and effective. Large-sample, prospective randomized controlled clinical trial and long-term oncologic outcomes are still required to make a comprehensive and objective evaluation of the use of posterior approach technique in LRH for cervical cancer.

![]()

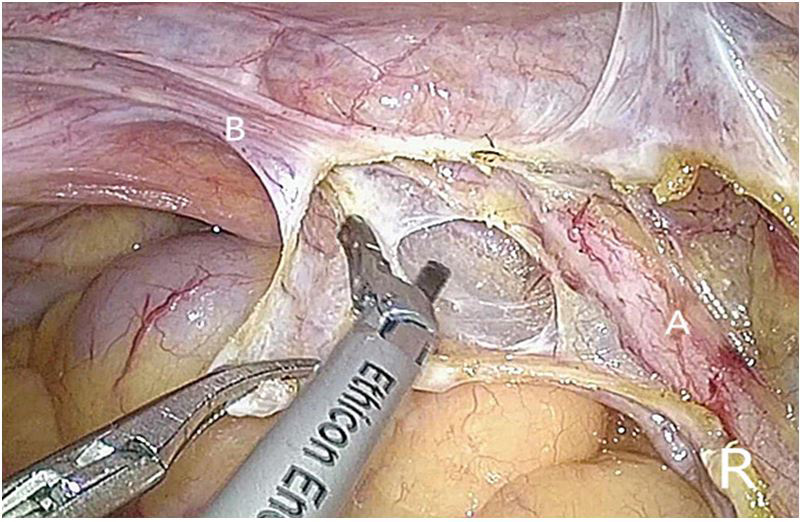 |
Figure 1: Macroscopic (A, C) and microscopic (B, D) aspects of patient’s lung and brain infected by C. deuterogattii, respectively (mucicarmin stain 400x) |
|
Figure 2: Agarose gel electrophoresis of URA5-RFLP after double digestion with Sau 96I and HhaI from C. deuterogatti clinical isolate. Left to right: MM: 50bp DNA ladder (Bionner, USA), VGI (WM 179), VGII (WM 178), VGIII (WM 161) and VGIV (WM 779), P (C. deuterogatti clinical isolate) |
|
Figure 2: Agarose gel electrophoresis of URA5-RFLP after double digestion with Sau 96I and HhaI from C. deuterogatti clinical isolate. Left to right: MM: 50bp DNA ladder (Bionner, USA), VGI (WM 179), VGII (WM 178), VGIII (WM 161) and VGIV (WM 779), P (C. deuterogatti clinical isolate) |
Characteristics |
Study group (n=23) |
Control group (n=27) |
p value |
Age (years) |
51.08±9.07 |
47.48±9.97 |
0.10 a) |
BMI (kg/m2) |
23.78±2.84 |
24.87±3.61 |
0.11 a) |
Histology |
|
|
0.55 b) |
Squamous cell carcinoma |
19 (82) |
23 (85) |
|
Adenocarcinoma |
4 (17) |
3 (11.11) |
|
Adenosquamous cell carcinoma |
0 (0) |
1 (4) |
|
FIGO stage |
|
|
0.39 b) |
Ib1 |
18 (78) |
17 (63) |
|
Ib2 |
3 (13) |
4 (15) |
|
IIa |
2 (9) |
6 (22) |
|
KPS score |
|
|
0.59 c) |
100 |
12 (52) |
12 (44) |
|
90 |
11 (48) |
15 (56) |
|
Data are shown as mean±standard deviation or number (%).
BMI, body mass index; FIGO, International Federation of Gynecology and Obstetrics
a)Student’s t-test; b)Pearson’sχ2 test; c)Mann-Whitney U test.
Table 1: Participants and tumor characteristics
Characteristics |
Study group (n=23) |
Control group (n=27) |
p value |
Operating time (min) |
248.96±42.66 |
282.22±81.45 |
0.15 a) |
Intraoperative blood loss (mL) |
185.42±193.64 |
296.30±201.40 |
0.04 a) |
The number of dissected lymph nodes |
20.96±7.75 |
21.93±6.72 |
0.44 a) |
Days of hospitalization (day) |
16.39±4.45 |
19.89±6.82 |
0.03 a) |
gastrointestinal exhaust time (day) |
2.65±0.71 |
2.52±0.80 |
0.47 a) |
catheter removal time (day) |
14.17±3.96 |
15.04±5.91 |
0.73 a) |
abdominal drainage tube removal time (day) |
6.35±3.01 |
8.07±4.41 |
0.09 a) |
Data are shown as mean±standard deviation or number (%).
a)Student’s t-test
Table 2: Surgical outcomes
Characteristics |
Study group (n=23) |
Control group (n=27) |
p value |
Intraoperative complications |
0 (0) |
0 (0) |
1.00 a) |
postoperative complications |
2 (9) |
5 (19) |
0.43 a) |
Ureteral fistula |
1 (4) |
1 (4) |
1.00 a) |
Pelvic infection |
0 (0) |
1 (4) |
1.00 a) |
Urinary retention |
1 (4) |
2 (7) |
1.00 a) |
None |
21(91) |
22 (81) |
- |
Clavien’s systematic classification of postoperative complications |
|
|
|
I |
0 (0) |
1 (2) |
1.00 a) |
II |
1 (5) |
3 (6) |
1.00 a) |
IIIa |
1 (5) |
1 (2) |
1.00 a) |
Data are shown as number (%).
a)Fisher’s exact test.
Table 3: Intraoperative and postoperative complications