Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2020 Chaudhary V. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background: Colporrhexis is separation of vaginal fornix from cervix and is a rare but serious cause of major obstetric haemorrhage in women during labor. Immediate clinical diagnosis is difficult but must be anticipated if haemorrhage continues despite contracted uterus following delivery. Rapid resuscitation and decision of laparotomy with either repair or hysterectomy is key in preventing maternal mortality.
Objective: We aim to present this rare case of colporrhexis with an insight to its risk factors and subsequent management
Case Presentation: A 28-year-old women Gravida 2 Para1 live 1 with previous caesarean section at 38+5 weeks of gestation with no other risk factors underwent spontaneous precipitous labor. She had spontaneous secondary incomplete colporrhexis with major obstetric hemorrhage, which was diagnosed early with immediate resort to obstetric hysterectomy.
Conclusion: Colporrhexis is a rare obstetrical emergency in modern obstetrics. Timely diagnosis, aggressive resuscitation, replacement of blood and blood products and early decision for laparotomy is key in preventing maternal morbidity and mortality.
Keywords:Colporrhexis; Cervical trauma; Hysterectomy; Vaginal birth after caesarean
Colporrhexis is defined as separation of vaginal fornix or upper one third of vaginal wall from cervix. It can occur both in pregnant as well as non-pregnant uterus. It can be primary or secondary to uterine rupture or cervical trauma following labor and delivery [1]. Clinical manifestations of secondary colporrhexis are similar to the rupture uterus. Early clinical diagnosis and resort to hysterectomy prevents maternal mortality. Colporrhexis is very rare with vaginal birth after caesarean section in 21st century due to improved obstetric care, appropriate selection of cases, presence of skilled obstetrician with careful monitoring during labor and delivery. We want to report a rare case of secondary incomplete colporrhexis following vaginal delivery in a patient of previous caesarean section.
A 28 yr. old, Gravida 2 Para1 live 1 at 38+5 weeks of gestation with previous caesarean section had with no other risk factors was admitted with chief c/o spontaneous intermittent pain abdomen for 2 hours. There was no leaking or bleeding per vaginum. Patient had uneventful antenatal course with no morbidity. She previous caesarean 3 years back in view of failed induction of labor with no complications. She had no significant past medical and family history. Her vitals were stable. Obstetrical examination showed term sized uterus in longitudinal lie with cephalic presentation .She was in latent labor .Her Per vaginal examination findings were 2 cm cervical dilatation with 70% effacement. Presenting part vertex was at -1 station with intact membranes and clinically adequate pelvis. After Informed consent she was admitted for trial of vaginal birth. She subsequently proceeded to second stage of labor within 3 hrs. and delivered healthy live baby of 2.7 kg vaginally. Her Predelivery investigations were Hb- 12.2gm/dl; Total leucocyte count – 6.6*103 per microliter, Platelet count 186*103 /microliter. Her biochemical profile was within normal limits. Following delivery heavy vaginal bleeding of around 500 cc was noted. As per Royal College of Obstetricians and Gynaecologists treatment of Postpartum haemorrhage protocol was started, continuous monitoring of vital signs, bimanual uterine massage, oxytocin infusion, labs for blood group typing and cross match, complete blood count, coagulation profile and kidney function tests were instituted. Bladder was catheterized which drained clear urine. Her oxygen saturation was 95% on room air. Her temperature was 97.6 degrees Celsius, Patient had tachycardia 120/min. BP 120/84 mm Hg. Mild pallor was noted. Uterus was 18 weeks, well contracted. On per speculum cervix appeared ballooned with intact walls. On pervaginum tense cervical ballooning was present and on negotiating os torrential hemorrhage of further 500cc was noted. Subsequently suprapubic bulge was noted with contracted uterus. Decision of examination under anesthesia due to suspicion of scar rupture / colporrhexis, was taken due to acuteness of event, and worsening clinical condition foregoing any imaging.
On examination under anesthesia, cervix was pulled up, upper right anterolateral aspect of cervix wasn’t visualized well and right lateral vaginal wall was congested. On per vaginum a very thin membrane like layer between the cervix and Right vaginal vault was noted, thereby differential of either uterine rupture or incomplete colporrhexis was made. Immediately, we proceeded to laparotomy. On opening the parietal peritoneum, uterus was intact, around 18 weeks size. Anterior bulge was seen along the lower uterine segment involving anterior cervix with bruising at the right vaginal angles with a layer of peritoneum intact (Figure 1). On further opening of visceral peritoneum and reflecting bladder downwards, right uterine artery along with descending branch was torn, contributing to hematoma of size 6X5 cm approximately. Upper Anterior lip of cervix was found to be damaged due to separation from vaginal vault, thereby confirming the diagnosis secondary incomplete colporrhexis.1 As involved cervix and vaginal area were unrepairable and there was ongoing hemorrhage, decision of obstetric hysterectomy was taken. Hemostasis was achieved. Total blood loss was 2.5 liters which was adequately replaced (4 units of fresh frozen plasma, 3 units of packed red cells). Her hemoglobin after replacements was 8.5gm% with normal platelet count and coagulation profile. Patient was discharged after stitch removal on 10 post op day in healthy condition.
Colporrhexis is defined as an avulsion of the vagina from the cervix. It is classified into primary or secondary, spontaneous or traumatic, complete or incomplete [1]. Incomplete colporrhexis includes rupture of the vaginal epithelium and the muscularis, and complete involves the overlying peritoneum. Primary colporrhexis is a vaginal vault tear not associated with cervical tear or uterine extension and is very rare. It constitutes 2.5% of all colporrhexis. Secondary colporrhexis involves either cervix or uterus but cannot be differentiated from a rupture that has originated in the uterus and then extended to involve the vagina [2]. Risk factors include high parity, unskilled instrumental delivery, precipitate labour and use of oxytocic’s in labour [3]. Excessive retraction of the uterus can tear the cervix from its vaginal attachment resulting in spontaneous colporrhexis [4]. A misdirection of the uterine axis due to a pendulous abdomen leading to marked anteversion of the uterus, ventrofixation of the uterus, evacuation of a full rectum after an enema, and prolapse leading to altered blood supply to the vagina are the other factors responsible [5].
Our case was secondary spontaneous incomplete colporrhexis (as visceral peritoneum was intact) with risk factor as precipitate labor. This was a rare case where scar and infravginal portion of cervix was intact but there was avulsion of supravaginal portion of anterior cervix from the underlying vaginal epithelium. and muscularis are involved [6]. In our case the rapid progress to second stage of labor led to shearing effect of the descending head on the upper vaginal wall and cervix, thereby tearing the descending cervical artery causing haemorrhage. As time proceeded with further haemorrhage and tear, cervix was retracted and anterior lip could not be seen on the repeat per speculum examination under anaesthesia.
In our patient we resorted to timely total hysterectomy, as there was a large hematoma beneath the intact scar involving lower uterine segment and cervix (secondary colporrhexis). Consultants were involved in the case from diagnosis till surgery. This also helped in rapid management of case. Early laparotomy with ongoing resuscitation is key in management of patients with colporrhexis in shock [7,8]. It helps in the assessment of the type of colporrhexis and timely surgical treatment, thereby preventing serious consequences of haemorrhage.
Colporrhexis is serious and life-threatening complication in mother following delivery. In women having hemorrhage following vaginal birth after caesarean, colporrhexis must be a differential diagnosis in addition to scar rupture. Early detection, resuscitation, involvement of senior obstetrician and early resort to laparotomy with hysterectomy are cornerstone in preventing the morbidity and mortality due to major obstetric hemorrhage which is a common feature in these cases.
The authors declare there was no conflict of interest

![]()

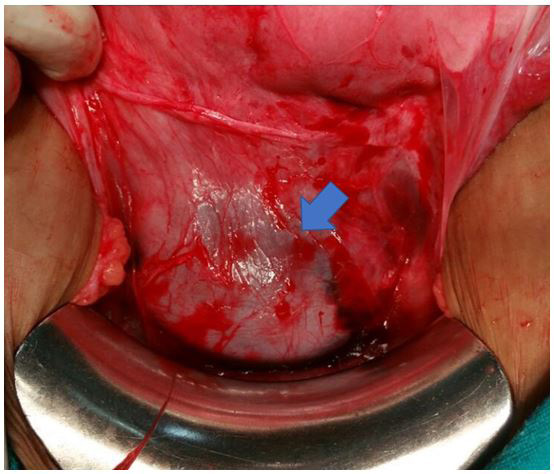 |
Figure 1: Anterior bulge (arrow) seen along the lower uterine segment involving anterior cervix |




































