Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2020 Ammar AS. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Gallbladder perforation presents in various forms with most common is the peritonitis. Most common causes include gallstones obstructing the cystic duct and necrosis of gall bladder due to ischemia.
Objective: We investigated whether a new ambulatory device is able to detect specific E-VOCs in patients with a medical history of cancer or dysplastic lesions and to which medical conditions they are associated.
Methods: All data were collected during routine consultations for Small Intestinal Bowel Overgrowth (SIBO). A breath test was performed by X-PID 9500®.
Results: 650 patients were included. 133 patients reported cancer or dysplasia. Three medical statuses associated with cancer/dysplasia were identifiWe report a case of 19-year-old female presented with history of abdominal distension for 4 months for which she was counselled to be because of pregnancy. She gave birth to healthy baby one month back but abdominal distension didn’t resolve. On examination, she had distended and tender abdomen with visible striae. Abdominal ultrasound showed a huge thick-walled cystic area with internal echoes measuring 31cm x 19cm x 19 cm with total amount of fluid volume in the cyst was approximately 5 liters arising from right hypochondrium. On opening the abdomen, a huge cyst was encountered extending from epigastrium to pelvis with dense adhesions. Cyst was opened and fluid aspirated. Communication between cyst was found with gall bladder inn the epigastrium. Cyst wall was excised partially and cholecystectomy done. Patient was discharged on 5th post-operative day.
The development of thick-walled huge cyst within abdominal cavity after gall bladder perforation is a rare entity specially when patient had gone through full term pregnancy in the presence of cyst.
Keywords: Case Report; Gall bladder; Perforation; Cyst; Pregnancy; Fistula
Gallbladder perforation is a rare presentation encountered in the surgical emergency floor [1]. The most common mode of presentation of gall bladder perforation is peritonitis but the pre-operative diagnosis of gall bladder perforation is difficult to made especially where there is no availability of advance imaging techniques like CT Scan [2]. This delay can result in morbidity and even mortality of the patient with significant influence on the outcomes. The reported incidence of gallbladder perforation in patients with acute cholecystitis is 2 - 18% while the incidence of gallbladder perforation because of acute cholecystitis is about 10 to 20%. The exact mechanism of gall bladder perforation in patients with acute cholecystitis is not understood [3]. In some patients of acute cholecystitis the impacted stone in the cystic duct fall back into gallbladder and this resolves the cholecystitis while if this inflammation don’t get resolved then persistent inflammation causes the development of empyema which inurn leads to necrosis and eventually perforation [4]. In most of the cases where perforation occur at fundus, omentum is least likely to cover the perforation so gross peritonitis occurs. On the other hand, if perforation occur at neck or the duct it is most commonly get sealed by omentum or the intestines which results in either local inflammation. The duration of symptoms may extend from one week to several months [5].
In this case report, we present a case report of 19-year female presented to surgical emergency department with sign and symptoms of huge intraabdominal cyst. The patient had history of spontaneous vaginal delivery of a full-term healthy child one month back. On exploration this huge intrabdominal cyst was communication with the fundus of the gall bladder and no stones were found in gallbladder or the cyst.
A 19-year-old female presented to the emergency department of EAST Surgical ward of MAYO Hospital Lahore, Pakistan in September 2020 with chief complaint of abdominal distension and off and on vomiting and fever for 4 months. She was married one year back and one month back she gave birth to a healthy baby through spontaneous vaginal delivery. On detailed history taking, she told to had experienced excruciating pain in right hypochondrium 4 months back for which she was counselled to be because of pregnancy and pain killers were given at a local village hospital. She took symptomatic treatment for off and on pain, vomiting and fever and gave birth to a baby one month back. After giving birth to the baby the abdominal distension remained the same with fever and vomiting for which she now presented to MAYO Hospital.
On examination, she had distended and tender abdomen with visible striae. She was tachycardiac with pulse of 124 per minute and blood pressure of 110/80 mmHg, normal respiratory rate, fever of 100-degree Fahrenheit and Glasgow Coma Scale of 15/15. She already had blood tests including complete blood count, liver function tests and renal function tests which were all in normal range and cytology of the fluid aspirated from the abdominal cyst from another hospital. Fluid cytology showed negative for malignant cells, neutrophils 95%, lymphocytes 5%, total leukocyte count of 17 x 109 /l. Chest x-ray and abdominal Xray erect was done which showed normal lung fields and diffusely increased density of the abdomen, poor definition of the soft tissue shadows, such as the psoas muscles, liver and spleen. Abdominal ultrasound showed a huge thick-walled cystic area with internal echoes measuring 31cm x 19cm x 19 cm with total amount of fluid volume in the cyst was approximately 5 liters arising from right hypochondrium. Because of the advantage of availability of CT Scan in the emergency department, CT Scan was done and it showed same findings as abdominal ultrasound with finding of superior part of the collection with the fundus of gall bladder, possibly secondary to the perforation of the gallbladder and causing mass effect on small intestines, urinary bladder and ureters (Figure 1). After resuscitation and giving broad spectrum antibiotics, plan of exploratory laparotomy was made after taking informed and written consent from the patient for exploration under general anesthesia and after arranging 2 pints of blood.
On opening the abdomen, the cyst wall is encountered just after cutting the peritoneum with layer of omentum overlying the cyst wall. The peritoneum was adherent to the cyst wall. After separating the peritoneum from cyst on both lateral sides, all of small intestine was found in left flank and large intestine on the right flank with dense adhesions. Cyst was occupying the whole abdomen form epigastrium to pelvis on both flanks. Lowers limit of the cyst was identified and cyst was opened by creating a small opening in the anterior wall of the cyst and about 6 liters of purulent fluid was sucked through the cyst. Cyst was then opened up to epigastrium where a small opening was observed which was communicating to the fundus of the gallbladder (Figure 2). The posterior surface of cyst was densely adherent to the aorta, major vessels and uterus and the posterolateral surface was adhered to colon so the wall of the cyst was excised up to the adhesions and rest of the cyst wall was left behind because of chances of iatrogenic injury to major vessels. In right hypochondrium gall bladder was identified with communication with the cyst and cholecystectomy was done. Single drain was placed in pelvis. Surgery and postoperative period remained uneventful and patient was discharged on 5th post-operative day and follow up was done for one month which was uneventful. Histopathology of the cyst wall showed acute on chronic cholecystitis and fluid from the cyst showed no evidence of malignancy (Figure 3 and 4).
Courvoisier first described 499 cases of gallbladder perforation in 1890 out of which 169 developed cholecysto-cutaneous fistulae. However, in past 50 years, less than 25 cases have been reported in the literature and this decline is mostly due to the inventions in advanced imaging techniques, surgical treatments and antibiotics [6]. Niemeier in 1934 classified gall bladder perforation into three types. Type 1 includes patients with free perforation into the peritoneum. Type II includes patients with localized perforation and type III includes patients with chole-cysto-biliary fistula and complex fistula formation [7].
Spontaneous gallbladder perforation or rupture is a well-documented complication of acute cholecystitis. The morbidity and mortality due to gallbladder perforation is estimated to be 57.7% and 9.5% respectively [8]. The most common age group affected by gall bladder perforation is between 48 to 60 years. Free perforation of the gallbladder is rare and the most common site of gallbladder perforation is fundus. Many case reports about gallbladder perforation are available in literature but still many controversies exist regarding the best tool for early diagnosis and the treatment modality [9]. Ultrasound abdomen is still the main investigation of choice in emergency and elective procedures but it can’t tell details about the perforation. For that CT Scan is the most sensitive tool to diagnose gallbladder perforation [10].
Perforation of the gallbladder can develop early in the course of acute cholecystitis or it may occur several weeks after the onset. Because of the poor blood supply fundus is the most common site of perforation [11]. Localized perforations can be found in literature but such a huge cyst with communication with the gall bladder is first of its kind [12].
This case is first of its kind and much different from the literature of gallbladder perforation available as in this case there is a history of about 4 months from the start of the symptoms and surprisingly no gross peritonitis occurred. Instead a well-formed thick wall was formed which was communicating with the gall bladder fundus. The secretions of the gall bladder were poured in the cyst for the last 4 months increasing the size of the cyst with the passage of time. The most interesting thing is that the patient got pregnant and delivered a healthy baby in between this condition.
Localized collection of the gall bladder perforation is reported in literature but a localized collection with well-developed thick wall extending up to the pelvis is first of its kind. Moreover, in the presence of such huge cyst patient also underwent pregnancy and delivered a healthy full-term baby. There were no sign and symptoms of peritonitis in 4 months of history. This case showed an unusual presentation of gall bladder perforation and this case add case report in the literature.
Written consent was taken from the patient.
The cluster 58 to 74.9s of E-VOCs is associated with cancer/dysplasia, especially of digestive origin. This cluster might be a good marker of gut-TH1-immunosuppression and vagal disturbances. The sensitivity of this cluster to identify patients with a medical history of digestive cancer or dysplastic lesions is 95.0%. The specificity is 82.8%. The positive predictive value is 43.7% and the negative predictive value is 99.2% which is quite performant for a non-expensive, ambulatory device and for a test which requires less than two minutes.
The cluster 58 to 74.9s appears to be rather a marker of severely altered physiological status with long term tissues consequences at the contact of inflammatory agents rather than of cancer per se or of mild-COVID-19 infection per se.
X-PID 9500® may become an ambulatory tool for detection of detection of increased risks of viral infection or cancer.
Further analyses are necessary to investigate where the inflammation associated with the cluster 58 to 74.9s takes place and which type of diet may trigger or abate it.
Ethical approval is not required at our institution to publish an anonymous case report.

![]()

 |
Figure 1: CT scan of the patient showing huge abdominal cyst. Arrow shows the communication between gall bladder and cyst |
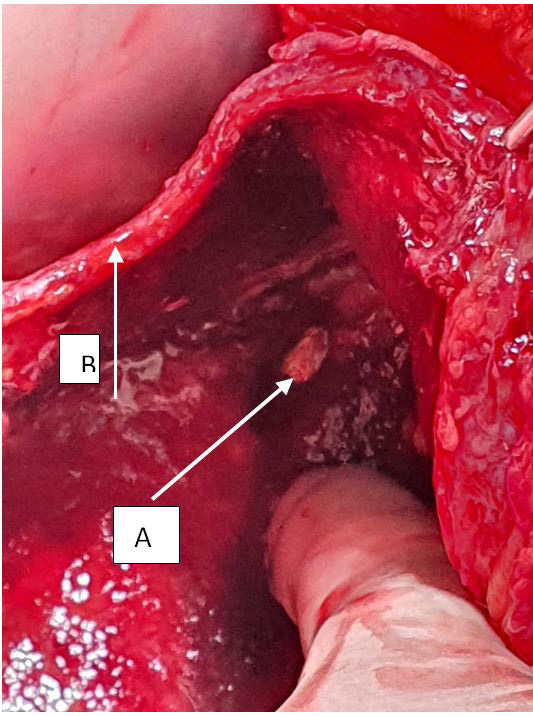 |
Figure 2: Inside view of the cyst after opening showing thickness of the cyst wall and communication with the gall bladder fundus; (A) showing communication of gall bladder with the cyst wall after opening the cyst; (B) showing the thickness of cyst wall |
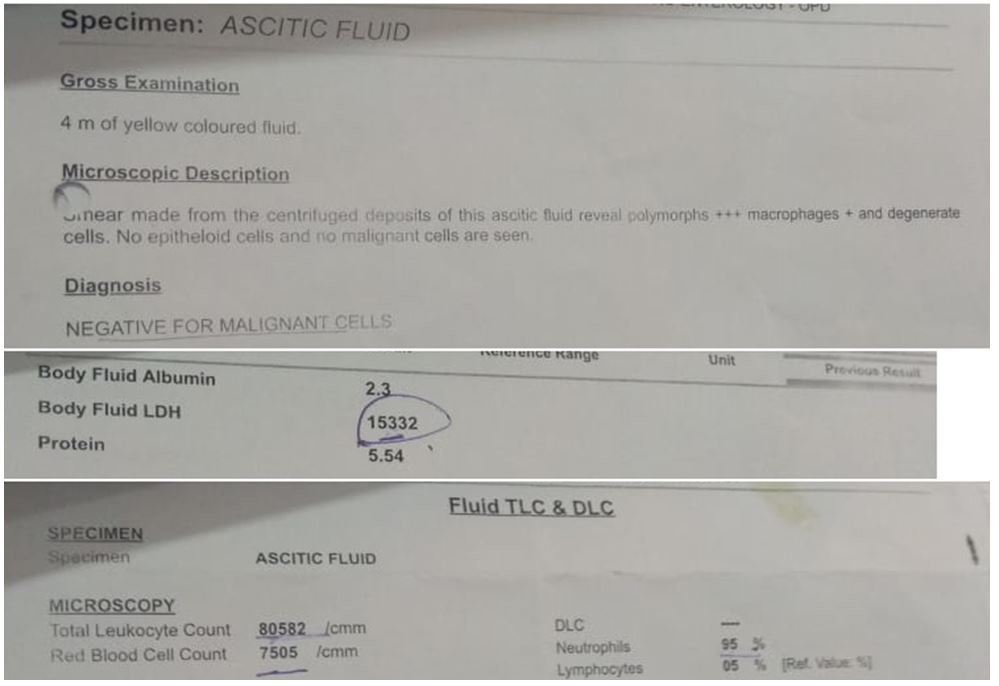 |
Figure 3: Fluid Cytology Report |
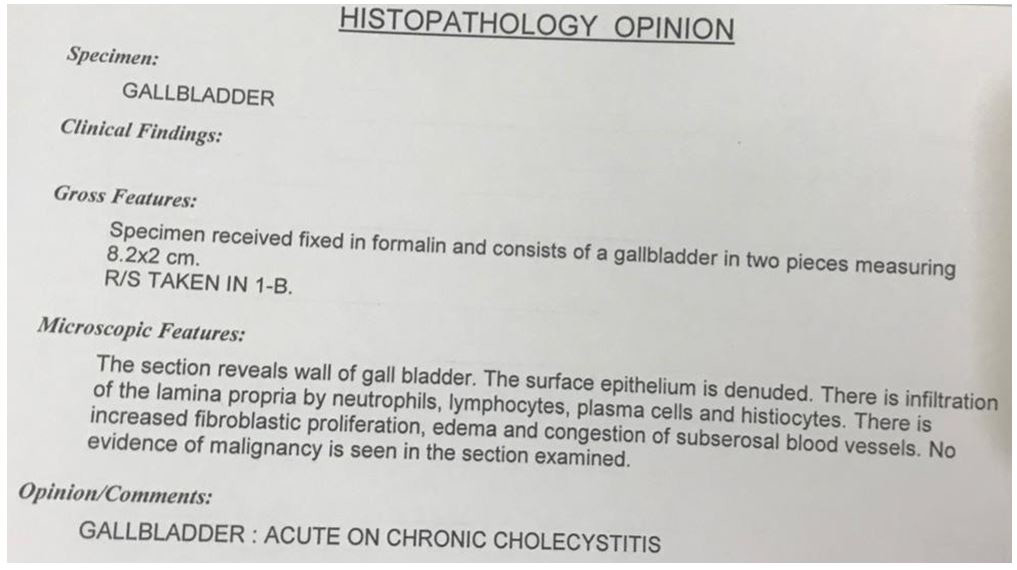 |
Figure 4: Histopathology report of the gall bladder |




































