Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2020 Lekhbal A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Amyloidosis is the finale pathway of a metabolic disorder in the body that can be primary or secondary leading to abnormal extracellular deposition of proteins in one or more tissues. Thyroid damage is very rare.
We report the case of a 61-year-old patient who was followed for bronchiectasis and presented an enlarged goiter with signs of malignancy. The biopsy of the mass led to the diagnosis of Amyloid goiter, which was revealing of the disease. Renal involvement was also subsequently confirmed. The patient was treated with colchicine, and the thyroid gland was preserved in the absence of signs of compression.
Amyloid goiter should be considered in any patient with goiter with a history of chronic inflammatory disease.
It is important to be aware of this entity, as the presentation varies widely and when diagnosed early the condition may be treated appropriately by relatively minor surgical intervention.
Keywords:Amyloid Goiter; Bronchiectasis
List of abreviations: AA Amyloidosis: Amyloid A Amyloidosis; MRI: Magnetic Resonance Imaging
The amyloid goiter, is a rare pathological entity due to the deposition of amyloid proteins in the thyroid gland, and causing an enlargement of the thyroid gland, may be secondary to a primary or secondary amyloidosis [1,2].
In the primary Amyloidosis, the kidneys, heart, nerves and gastrointestinal system are the organs most affected. In the secondary Amyloidosis the spleen, liver, kidneys, adrenal glands are the most affected [3].
Thyroid treatment is surgical when the patient presents signs of compression.
We report the case of a woman whose amyloid goiter was the first manifestation of a secondary amyloidosis.
We describe the case of a 61-year-old woman, followed for bronchiectasis since 9 years under treatment (inhaled corticosteroids). The patient had presented a previous cervical swelling since 6 years, this mass has progressively increased in volume, without signs of compression, or dysthyroidism, and without alteration of the general state of health. Examination found a large cervical mass at the expense of the thyroid (Figure 1), fixed in relation to the superficial and deep planes, and without cervical lymphadenopathy, nasofibroscopy showed normal mobility of the vocal cords. The patient benefited from a cervical ultrasound scan which showed the presence of multiple nodules in both lobes, the largest one measuring 28mm long axis and classified EUTIRADS 4, the imaging was completed by a cervical MRI which objectified an enlarged thyroid gland, not plunging, and strongly raised and heterogeneous after gadolinium injection (Figure 2). The biologic evaluation found a normal thyroid function (TSHus=2,85 mUI/l), but renal function was impaired (creatinine=54,30/ MDRD= 5,32 ml/mn).
In view of the fixity of the mass, a biopsy was recommended under local anaesthesia. On anatomopathological examination with immunohistochemical study after staining to Congo red, amyloid deposition expressing amyloid A protein was found. The patient was subsequently referred to nephrologists who performed a renal biopsy which was in favor of the same diagnosis.
The patient was placed on colchicine 1mg/ day with thyroid gland preservation.
Amyloidosis is a condition of unknown etiology. There are several types of amyloidosis, including secondary generalized amyloidosis, which consists mainly of AA protein, and in which all organs can be affected, including the peripheral nervous system, the thyroid is rarely affected [4].
It is a infiltration by amyloidosis deposits very frequently observed in systemic amyloidosis, these deposits are asymptomatic and do not cause goiter or dysthyroidism in the majority of cases, and found on a specimen of thyroidectomy or autopsy [5]. Indeed, the quantity of amyloid deposits is rarely sufficient to modify the volume of the gland.
Clinically, the amyloid goiter is often compressive and can therefore simulate a thyroid cancer as it was revealed in our patient [6]. Patients may be in hypothyroidism, hyperthyroidism, or euthyroidism [2,4], our patient was in euthyroidism.
The diagnosis of an amyloid goiter can be made by a simple cytopunction, but it is difficult to make a differential diagnosis with a medullary carcinoma, which is why the diagnosis is mainly histological on the surgical specimen [7].
There is no effective treatment for systemic amyloidosis. Colchicine can prevent the progression of amyloid deposits in AA amyloidosis, but the effectiveness of this treatment is still debated [8].
SFor the thyroid gland the choice therapy is total thyroidectomy if there are signs of compression [9].
The diagnosis of amyloid goiter should be considered in any goiter patient with a history of chronic inflammatory disease.
Informed consent was received from the patient.
All authors have no conflict of interest or financial support with this article.

![]()

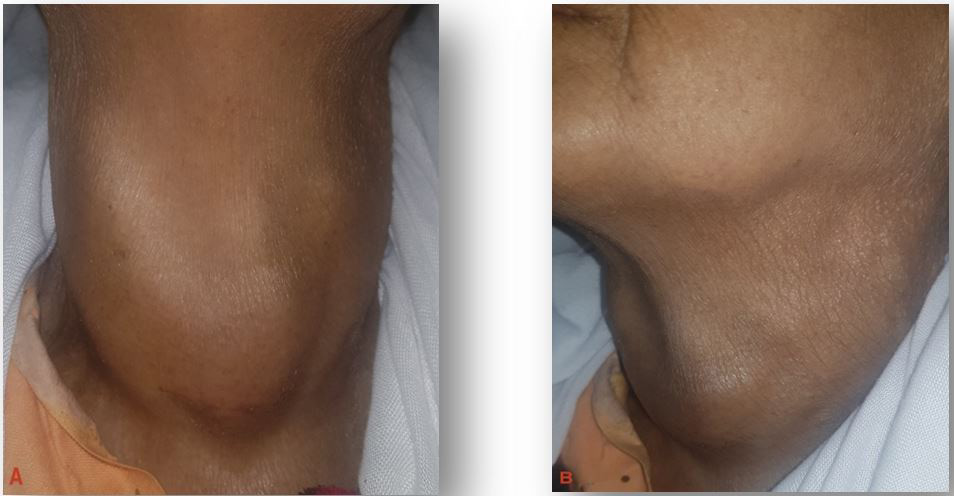 |
Figure 1: Appearance of the mass on a front (A) and side (B) view, showing the voluminous goiter with a postoperative scar of the cervical incision |
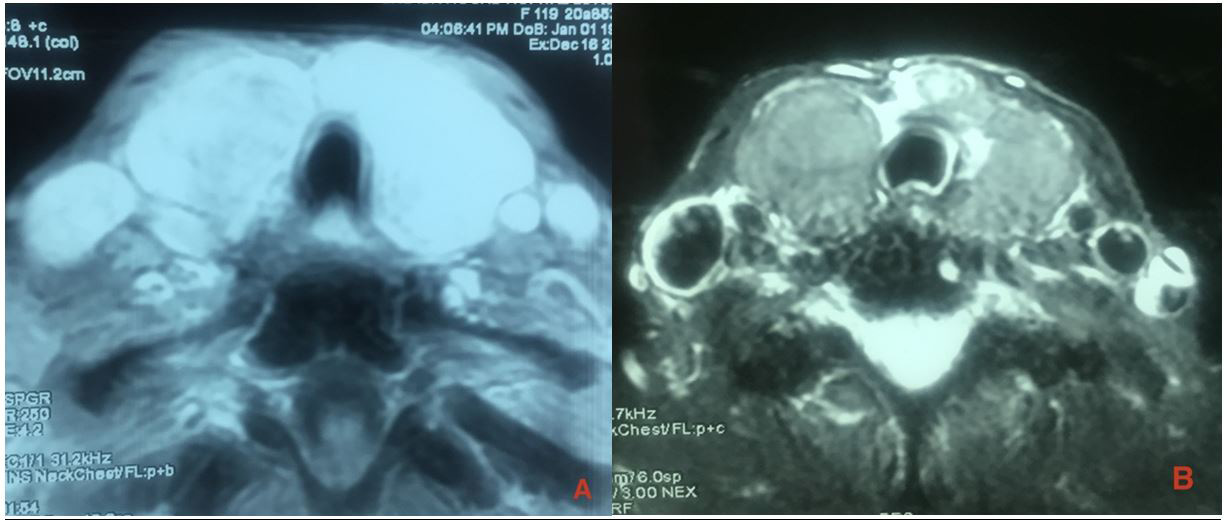 |
Figure 2:Cervical MRI (A: T2 with injection; B: T1) which objectified an enlarged thyroid gland, and strongly enhanced intensely and in high heterogeneous after gadolinium injection |




































