Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2020 Ettanji A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
In the adult population, the incidence of urachal anomalies is approximately 1 in 5000 with a higher prevalence in men. Urachal abscess is an uncommon condition with protean features and often presents a diagnostic challenge to clinicians.
We report a case of a 42 year old man that presented with a urachal complex mass which, after proper investigation, was revealed to be a huge urachal abscess.
Surgical excision is the therapeutic mainstay of the urachal abscess, but preoperative management approach often varies.
It is important to be aware of this entity, as the presentation varies widely and when diagnosed early the condition may be treated appropriately by relatively minor surgical intervention.
Keywords:Urachal; Abscessed; Pyourachal; Cyst
The urachus is a fibrous cord structure formed after the obliteration of the urogenital sinus and allantois during the embryologic process. The urachal canal normally obliterates as the bladder descends into the fetal pelvis, forming a fibrous connection with the ventral abdominal wall known as the median umbilical ligament. Complete obliteration typically occurs during late fetal development or early infancy (6 months) [1].
Abnormal remnants of the urachus can present as patent urachus, vesico urachal diverticulum, urachal sinus or urachal cyst.
In the adult population, the incidence of urachal anomalies is approximately 1 in 5000 with a higher prevalence in men [2]. Urachal abscess is an uncommon condition with protean features and often presents a diagnostic challenge to clinicians.
The treatment of choice of a urachal abscess in the adult patient includes broad-spectrum antibiotics and drainage, if necessary, as initial therapy. Surgical excision is recommended after the resolution of the infection because there is a 30% reinfection rate and a risk of malignant degeneration of an unresected or incompletely resected urachal remnant.
We report a case of a 42 years old man that presented with a urachal complex mass which, after proper investigation, was revealed to be a urachal abscess.
We describe a case of 42 years old man, with no relevant past medical history, who presented with 2 months history of hypogastric mass associated with fever, diarrhea, weakness and decreased appetite.
The physical examination revealed a febrile man (38°c) with correct vital signs and a 15 cm hypogastric erythematous mass, painful and warm upon palpation, without umbilicus pus issue or pyuria. Signs of peritonism were absent (Figure 1).
At that point, a lesion of the urachus was suspected. However, it was not clear whether it was a urachal abscess or carcinoma.
Initial laboratory data revealed a WBC count of 41000/mm3, hemoglobin count of 13,2 g/dl, and an elevated C-reactive protein level of 143,1 mg/l, others were within the normal limit.
An abdominal ultrasonograph study revealed a huge hypogastric mass with heterogeanous content.
A computed tomography scan of the abdomen and pelvis was performed, and represented a large extra peritoneal collection extend from umbilicus to pubis, with an infiltration of the surrounding soft tissue. This collection measures 16 x 15.5 x 9cm. There was no evidence of communicating between the abscess cavity and the bladder (Figure 2).
Drainage with a joly drain was performed under local anesthesia and then, intraveaunous antibiotics and the drain were maintained for 2 weeks. The bacteriological sampling revealed an E. coli.
After a marked clinical and biological improvement, with a correct WBC count and normal C-reactive proteins, an infra-umbilical midline laparotomy was performed. The operative finding revealed that the abscess was derived from an urachal duct cyst. The urachal abscess and remnants were dissected inferiorly to confirm no communication with the bladder before total excision. However, recently, the laparoscopic method has been accepted as an alternative option because of faster recovery, less postoperative pain and better cosmetic results.
During normal development in the embryological life, the luman of the urachal closes and separate it from the bladder by the valve of Wutz. In up to one-third of individuals the lumen remains patent. Rarely anomalies result from failure of closure of the urachal lumen [3].
The urachal cyst is the most commonly regarded anomaly of the failure of close urachal. If the cyst remains steril it may be asymptomatic until it became larger or infected.
The urachal disease is usually diagnoses in childhood, it is rare in adults. Yiee and al. reported that there were approximately two cases of urachal abnormality per 100,000 hospital admissions in adults.
An urachal abscess classicly presents as a tender, lower midline abdominal mass. Overlying erythema is often associated. Systemic signs of infection, including fever, malaise and leukocytosis, are present. The clinical course may a spontaneaous drainage into the bladder, or in rare cases the abscess my perforate into the peritoneal cavity, causing an acute surgical abdomen.
Ultrasound appears to be the first line choice in patients who present an abdominal wall mass. A CT scan is the gold standard and recommended for adult patients so as not to miss a tumor and also to search for a communication between the urachal abscess and the bladder if objectified by a passage of the contrast medium into the cavity of the abscess.
Surgical excision is the therapeutic mainstay of the urachal abscess, but preoperative management approach often varies. Some follow the two-stage management approach, treating the infections with antibiotics and drainage of the abscess before surgical excision. Others prefer removing directly the urachal abscess [4,5].
Our patients, received antibiotics and drainage first, than after the resolution of the infection a surgical excision was performed without experiencing any postoperative infectious complications.
Another variable influencing surgical management for urachal disease is the perceived risk of malignancy. Urachal carcinoma is rare but with poor prognosis. An investigation of 130 adults cases from 1951 to 2005 revealed that 51% of urachal specimens were malignant [6].
The diagnosis of an acquired urachal abscess is difficult and may be confused with variety of surgical, urological and gynecological conditions. It is important to be aware of this entity, as the presentation varies widely and when diagnosed early the condition may be treated appropriately by relatively minor surgical intervention.
The author(s) indicated no potential conflicts of interest.

![]()

 |
Figure 1: Hypogastric mass |
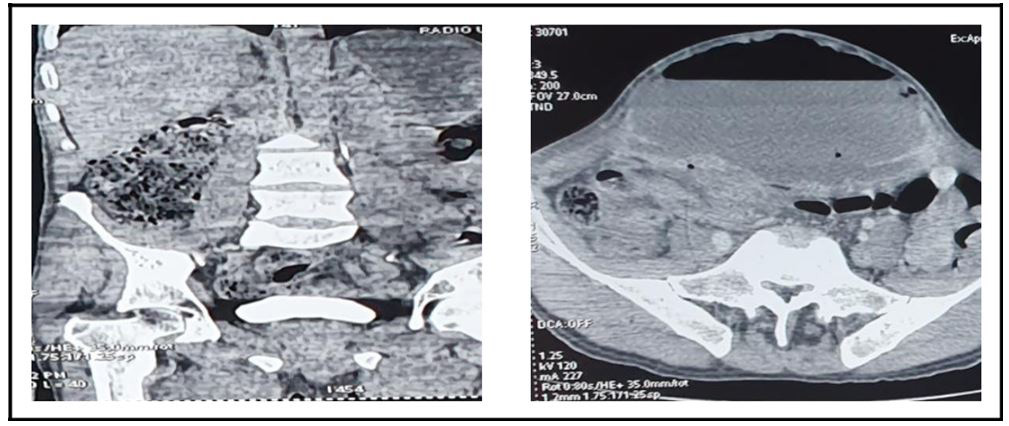 |
Figure 2:Computed tomography showed huge abscess containing fluid and gasDiscussion |




































