Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2020 Cambron J. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Intrauterine devices are one of the most common and effective versions of contraceptive. There have been many reports in the past of these devices perforating the uterus and being found in the bladder, peritoneum, and colon to name a few. In this paper we present the case of a woman who presented to the emergency department with severe hydronephrosis and associated pyelonephritis as result of intrauterine device migration into the patient’s fallopian tube causing ureter compression. Interestingly, she had also given birth to two healthy infants since having intrauterine device placed and assumed that it had fallen out years prior. To the best of our knowledge there have been very few such cases reported in the literature.
Keywords:Emergency; Migrated Intrauterine Device; Obstructive Uropathy
Intrauterine devices are a common long acting birth control known to be one of the most effective available tools for reversible contraception [1,2]. Complications related to intrauterine device insertion are rare in general and in terms of myometrium injury and uterine perforation the incidence rate is as low as 0.01% [3]. Known risk factors for intrauterine perforation include placement within 6-month postpartum period, postpartum amenorrhea, and inexperienced providers [3,4]. We present a case of hydronephrosis and pyelonephritis in a 25-year-old woman due to migration of intrauterine device into the fallopian tube causing mechanical compression of adjacent ureter. Interestingly, the patient has had multiple heathy children since placement and migration of intrauterine device.
A 25-year-old G5P5 (all vaginal births) female presented to the Emergency Department with left sided flank and left lower quadrant abdominal pain. She denied any other complaints. The pain began earlier that same day and she denied any previous similar symptoms. She denied any significant past medical or surgical history. Vitals revealed mild fever of 99.9, tachycardia with heart rate of 108 and blood pressure of 119/80. Physical exam noted a young woman uncomfortable in appearance and was positive for left flank tenderness and left lower quadrant abdominal tenderness to palpation but otherwise negative. Laboratory workup revealed leukocytosis with WBC of greater than 17,000 and Urinalysis consist with urinary tract infection due to 2+ Leukocyte Esterase and WBC/Bacteria labeled by our laboratory team as Too Numerous to Count. Patient then underwent Cat Scan of abdomen/pelvis revealing severe left sided hydronephrosis with associated perinephric fat stranding consistent with pyelonephritis (Figure 1). Interestingly, it was also noticed that the patient had an apparent intrauterine that had migrated within the left pelvis, possible within left fallopian tube and was compressing the left ureter (Figure 2). The patient then revealed that she had an intrauterine device placed three years ago but had assumed it had fallen out due to her two successful pregnancies following intrauterine insertion. Patient was then admitted to OB/Gyn and Urology services. Retrograde Pyelogram revealed and intact ureter with noted stricture at presumed location of intrauterine compression. At this time a JJ ureteral stent was placed by Urology. While admitted the patient received ongoing intravenous antibiotic treatment with scheduled Rocephin and improved quickly. OB/Gyn services then performed laparoscopic removal of the intrauterine device which had perforated the fallopian tube and was placing direct compression on the left ureter. The intrauterine device was removed without difficulty. The patient recovered quickly after being discharged with two-week course of outpatient Ciprofloxacin.
Intrauterine devices are commonly used in birth control with over 99% effectiveness and a low side effect profile. Although rare a known side effect is intrauterine device migration outside of the uterus [5]. The migrated intrauterine device can be found in locations such as the omentum, appendix, colonic lumen, myometrium, bladder, pouch of Douglas and the retroperitoneum [5-11]. There have been many case reports in the past demonstrating intra-vesicular migration of intrauterine device and subsequent complications [6-8,10]. Obstructive uropathy related to pathologic migration of an intrauterine device is an extremely rare presentation, with very few demonstrations in previous literature [12]. Our case was made even more unique by the fact that the patient had developed pyelonephritis, was successfully treated with antimicrobials, and had two successful full-term pregnancies and deliveries with the migrated intrauterine device present. This stresses the importance of removal of these migrated intrauterine devices once detected even if they are asymptomatic as they may result in future complications [5,13,14].
In conclusion, this case presents a rare presentation of severe hydronephrosis and associated pyelonephritis related to intrauterine device migration. This case stresses the importance of device removal if migration has occurred as well as reminding emergency physicians to have a low threshold for further investigation in women with possible intrauterine device complications.

![]()

 |
Figure 1: Severe Right sided hydronephrosis with associated fat stranding consistent with pyelonephritis |
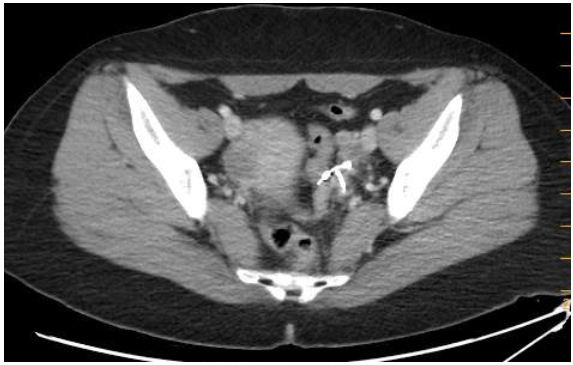 |
Figure 2:Intrauterine device seen within left lower abdomenReferences |




































