Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2019 Habib M. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Guide wire fractures during coronary or peripheral angioplasty are very rare and Incidence of these complications are around 0.02 % [1]. The guide wire remnants can lead to complications, such as thrombosis, embolic phenomena and perforation [2].
There are several methods recommended for the management of fractured guide wires, including snare removal, emergent surgery, Triple wire technique, stent deployment over a severely angulated guide wire and conservative treatment [3-5].
We present a case broken guidewire filament that successfully removal by grasping forceps after failure of several attempt of snare device to remove remnant segment.
Keywords:Percataneous Peripheral Angioplasty; Guidewire Fracture; Grasping Forceps
A 62-year-old male patient presents with acute left leg pain, underwent lower limb artery angiography because of lower limb ischemia at rest. Diagnostic catheterization performed from the right femoral artery by 6 french sheath, the left lower limb angiography suggested that Common iliac artery 70% stenosis, Common femoral artery 80% stenosis and superficial femoral artery mid long segment totally occluded by thrombus (Figure 1).
Angioplasty for left superficial femoral artery was planned, Judkins right 3.5, 6 french guiding catheter was inserted from right femoral. Then angioplasty 0.014 guidewire was inserted (hi-torque Balance Middleweight (BMW) universal coronary guide wire, Abott Vascular, Santa Clara, CA, USA) into right femral artery and advanced into left superficial femoral artery. During attempts to retract the BMW wire positioned in the vessel, it became apparent that the distal radio-opaque portion of the wire was fixed in the mid superficial femoral artery. With continued retraction, there was subsequent unraveling and fracture of the guidewire (Figure 2).
We use snare to removal broken guidewire. We tried several attempts to snare it out, but was unsuccessful (Figure 3).
Then we inserted another femoral sheath from left femoral artery (anterograde type) and we used a Grasping Forceps (Karl Storzs) - usually used to retrieve foreign bodies from the respiratory system by the ENT specialists - to catch the tip of the broken guidewire. After few maneuvers we were able to catch the distal tip of the broken guide wire which was pulled back into the tip of the sheath; then everything was pulled back together successfully (Figure 4).
Then we inserted pilot 50, 0.014 inch coronary guidewire from The femoral artery was entered with 6 Fr. Sheath, and positioning Judkins Right 4, 6 French guiding catheter in the left femoral artery, then the lesion was crossed by 0.014 inch pilot 50 guidewire and placed in the distal popliteal artery with free movement of the tip. Patient was pretreated using 325 mg Aspirin, 600 mg Clopidogrel and bolus intravenous 10.000 U Heparin. Then four 4x30 mm Zeta stents were deployed at 14 atmospheres (Figure 5). At the end of the procedure, there was no residual stenosis, dissection or evidence of an aneurysm and there was good flow in the stented femoral artery (Figure 6).
Hi-torque BMW guide wires consist of a distal core and a stainless proximal shaft, facilitating treatment of multiple lesions and tortuous vessels. However, guide wire fractures may occur if the distal core and stainless proximal shaft are separated by either the trapping of the distal tip or by vascular resistance.
Anticoagulation or antiplatelet agents are additionally used in this setting to prevent the subsequent development of thrombosis. Successful emergent surgery has been performed [6]. Various methods for extraction of fractured materials are available. Snares of various types have been utilized including gooseneck snares and loop snares [7,8] which are more suitable for proximal, large-caliber vessels.
Stenting over the retained device is another option in a vessel of a suitable diameter when appropriate equipment can be delivered [9].
Conservative therapy may be appropriate for small, occluded vessels; it was not felt to be appropriate in this setting due to the risk of propagation of thrombus to the proximal component of the unraveled guide wire.
To our knowledge, this is the first such case reported to using this Grasping Forceps successfully after failure of dedicated snare devices which allowed the patient to avoid major surgery. At the end it is left for me to mention that all this work was done in a center without on site surgery.
Awareness of the suitability, advantages and limitations of the various described techniques for fracture wire retrieval, as well as the role of conservative management and emergent surgery, is critical. The use of Grasping forceps to removal the fractured guidewire is a simple and straightforward method, and is potentially a valuable tool in the management of these complications.

![]()

 |
Figure 1: (A) common iliac artery 70% stenosis; (B) Common femoral artery 80% stenosis, (C) superficial femoral artery mid totally occluded |
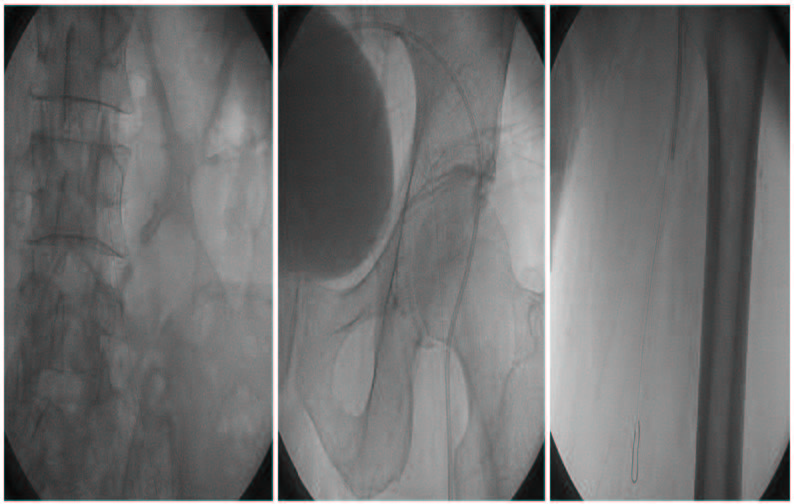 |
Figure 2: Guidewire fracture at ostial left common iliac artery with reminant from ostial common iliac artery to mid superficial femoral artery |
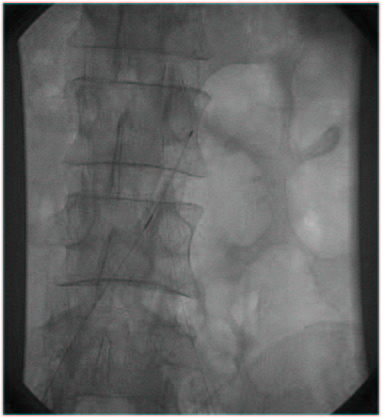 |
Figure 3: The snare in the abdominal aorta to catch broken guidewire |
 |
Figure 4: Removal broken guidewire by Grasping forceps |
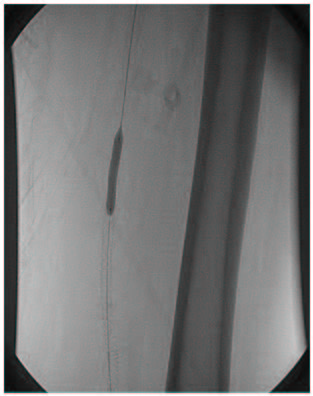 |
Figure 5: Stent deployed in superficial femoral artery |
 |
Figure 6: Superficial femoral artery after 4 stent |




































