Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2019 Hadadi H. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background: Glioblastoma is the most common and most deadly type of primary brain malignant tumors. despite applying the best trimodal treatment consisting of surgery chemoterapy and radiotherapy, there are few patients who survive decades after treatment.
Case presentation: In 2006, a 40 year-old man had been suffering from headache and convulsions, was operated for a glioblastoma in the right fronto-parietal lobe. After the operation the patient underwent partial-brain radiotherapy. Ten years after surgery the patient has local recurrence of the tumor, completely removed by second surgery. Today, 3 years later he still recovery from glioblastoma.
Conclusion: Long-term survivors represent a very exceptional group of patients with glioblastoma. A survival of 0 years or more has been reported sporadically over the last 50 years, which should serve as a stimulus to continue the research therapies against this tumor and increases chances of reaching recovery without recurrence.
Keywords:Glioblastoma; Resection; Long-survival; Recurrence; Chemotherapy; Radiotherapy
List of abbreviations: MRI: Magnetic Resonance Imaging; CT: Computed Tomography; RT: Radiation Therapy; CBTRUS: Central Brain Tumor Registry of the United States; OS: Overall Survival; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; MGMT: O6-methylguanine-DNA methyltransferase; IDH: Isocitrate Dehydrogenase
IGlioblastoma is the most common and most deadly type of primary brain malignant tumors. The cancer registry in Morocco has no data on the incidence of the central nervous system. Despite applying aggressive multimodality approaches with maximum safe resection, adjuvant radiotherapy and temozolamide, prognosis for this malignancy remains very poor: most patients die within 2-8months from diagnosis [1,2]. There is however 3-5% of patients who survive 5 years or longer and are referred to as long-term survivors [3-6]. We describe the case of one of some exceptional patient with glioblastoma who survived more than 2 years after the initial complete resection and adjuvant radiotherapy.
In 2006, a 40 year-old man had been suffering from headache and convulsions for about a month. A MRI scan showed a tumor in the right fronto-parietal lobe, this lesion measured 80x40 mm and was hypo intense signal in T weighted images with low enhancement and hyper signal in T2 weighted images (Figure 1).
The Patient underwent stereotaxic biopsy and then surgery; the tumor was removed seemingly in-toto. Histological report showed the neoplasia to be a glioblastoma (Figure 2). The patient’s postoperative course was uneventful. The patient was referred to our department for radiation therapy. A total dose of 59.4Gy was delivered with 1.8 Gy per fraction (5 fraction per week). The treatment was in general well tolerated.
A first CT scan, Three months after radiotherapy, showed no signs of active disease. Since then, he has had regular scans (CT or MRI), further and further apart in time (Figure 3). In 206, the patient had again headache and epileptic crisis without neurologic symptoms. A MRI scan showed right frontal hyper intense signal T2 weighted and FLAIR images and a recurrence was highly suspected (Figure 4). The patient underwent a tumor resection and the histologic examination revealed anaplasic oligodendroglioma with IDH mutation and chemotherapy with six cycle of temozolomide. Today, 3 years later he still controlled (Figure 5).
Glioblastoma is the most common type of malignant brain tumor in adults. Most of patients affected by this malignancy are managed with a combined-modality approach, incorporating adjuvant postoperative radiation therapy (RT) and adjuvant chemotherapy following initial surgery. Even with Stupp protocol, extent of resection and new radiotherapy techniques, median survival, doesn’t exceed 2–8 months from diagnosis [-6], with less than 2.6% surviving more than 0 years according to the report from the Central Brain Tumor Registry (CBTRUS) of the United States in 2007 – 2011 [7].
A 0-year survival after glioblastoma diagnosis, namely more than a decade, has been described in individual cases over the last 50 years [8-11] but no explanation predictive of a favorable prognosis has been identified. Our case also survived for more than 0 years even with recurrence after 0 years of the initial complete resection. We can’t give any exact reason of the longer survival in our patient. There are many possibilities, but the most probable explanation may be the younger age of our patient and complete resection of the tumor at initial and second operation.
Long-term survival or decade survivors tend to have neoplasm in the cerebral hemisphere and are relatively young. Analysis of the possible factors affecting the prognosis for patients with glioblastoma showed that age was one of the single most important prognostic factors [1,12]. The data from a CBTRUS extracted glioblastoma in age groups revealed significantly superior prognosis in younger patients. The 0-year overall survival (OS) in the groups of 0–4, 5–39 and 40+ years were 4.9%, 3.6% and .6% respectively [7]. The location and age of our patient may have affected the prognosis, but the exact reason remains more complicated than that.
The safe maximal resection is another important factor significantly affecting the prognosis in glioblastoma. Brown et al. in the largest meta-analysis on the correlation between extent of resection and survival; showed that survival was better after a total resection comparing to a subtotal resection [13]. They also found that the chance of a 2-month PFS increased by 5% after a total resection. In a recent systematic review conducted in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline by T. Tykocki and M. Eltayeb in 2018 [14], reported that the majority of long-term survivors had a total resection. Our case also had complete resection of the neoplasm which is consistent with the general trend presented in literature.
Some authors have related long-survival after maximal resection to the molecular characteristics of glioblastoma, for example the absence of epidermal growth factor receptor gene amplification, the presence of O6-methylguanine-DNA methyltransferase (MGMT) promotor hypermethylation, isocitrate dehydrogenase (IDH) mutation [3]. Our patient also had IDH mutation after examination of the second tumor resection. The presence of an IDH or IDH2 mutation confers a two- to threefold improvement in survival compared with IDH-wildtype tumors. In a study that included more than 400 gliomas, the presence of an IDH mutation was associated with significantly improved median survival in grade II gliomas (5 months vs 60 months), grade III gliomas (8 months vs 9 months), and glioblastomas (27 months vs 4 months) [16].
Long-term survivors represent a very exceptional group of patients with glioblastoma. Despite improved combined-modality approach, this malignancy continues to be regarded as incurable and universally fatal. A survival of 0 years or more has been found to be less than 2.6% in the population of glioblastoma cases, which should serve as a stimulus to continue the research therapies against this tumor and increases chances of reaching recovery without recurrence.
The authors would like to thank the team of radiation therapists for performing daily image control before the treatment, and the social department of Moroccan Royal Armed Force for patient’s psycho social support.
Written informed consent was obtained from the patient for publication of this Case Report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Khalid Hadadi and Abdelhak Maghous were the major contributors in writing the manuscript. El Amin Marnouche, Noha Zaghba, Khalid Andaloussi, Mohamed Elmarjany, Khalid Hadadi, Hassan Sifat and Hamid Mansouri cared for the patient during her time in the hospital and assisted in data collection and the preparation of the manuscript. All authors read and approved the final manuscript.
We wish to confirm that there has been no significant financial support for this work that could have influenced its outcome.

![]()

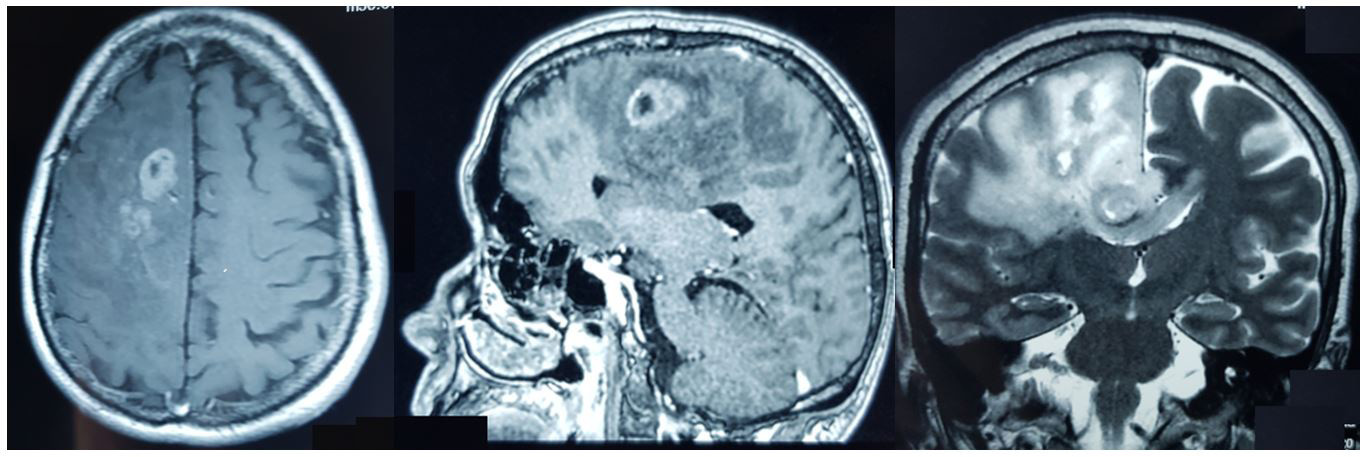 |
Figure 1: T2 coronal MRI sequence and T1-weighted axial and sagittal gadolinium-enhanced MRI showing a tumor in the right fronto-parietal lobe |
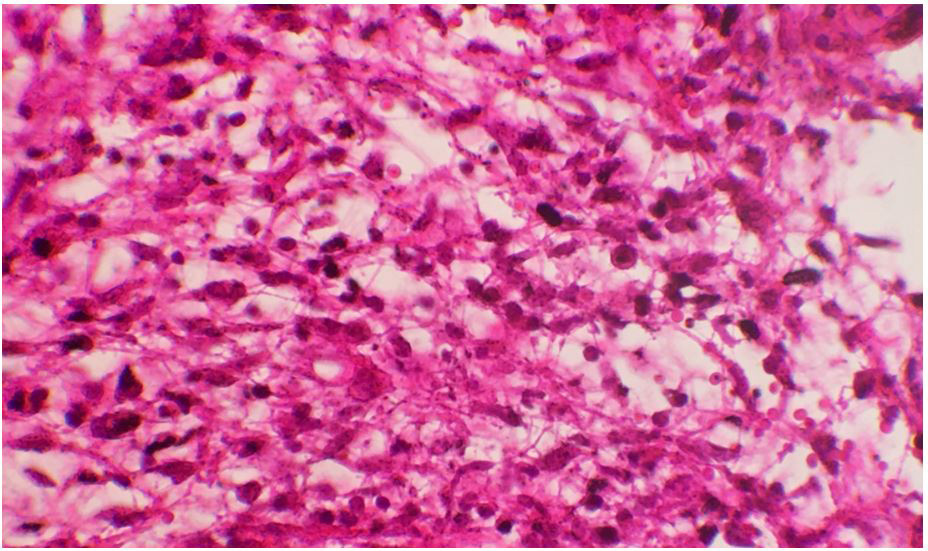 |
Figure 2: Dense proliferation of atypical astrocytic cells with blanks of necrosis (HEx40) |
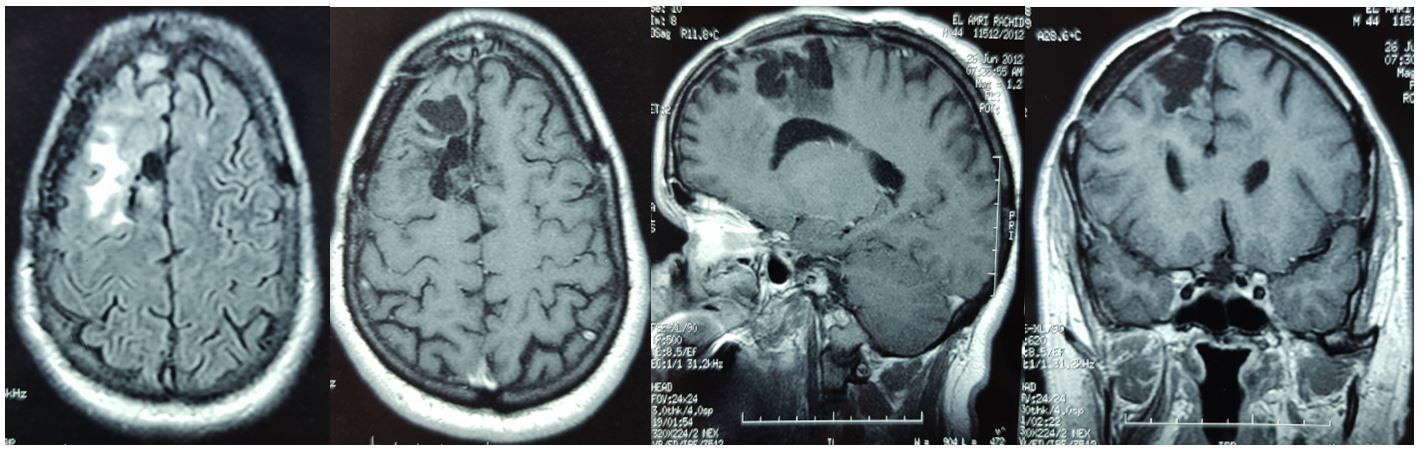 |
Figure 3: T2 axial MRI sequence and T1-weighted axial, sagittal and coronal gadolinium-enhanced MRI without enhancement and tumor residue six years after initial complete resection |
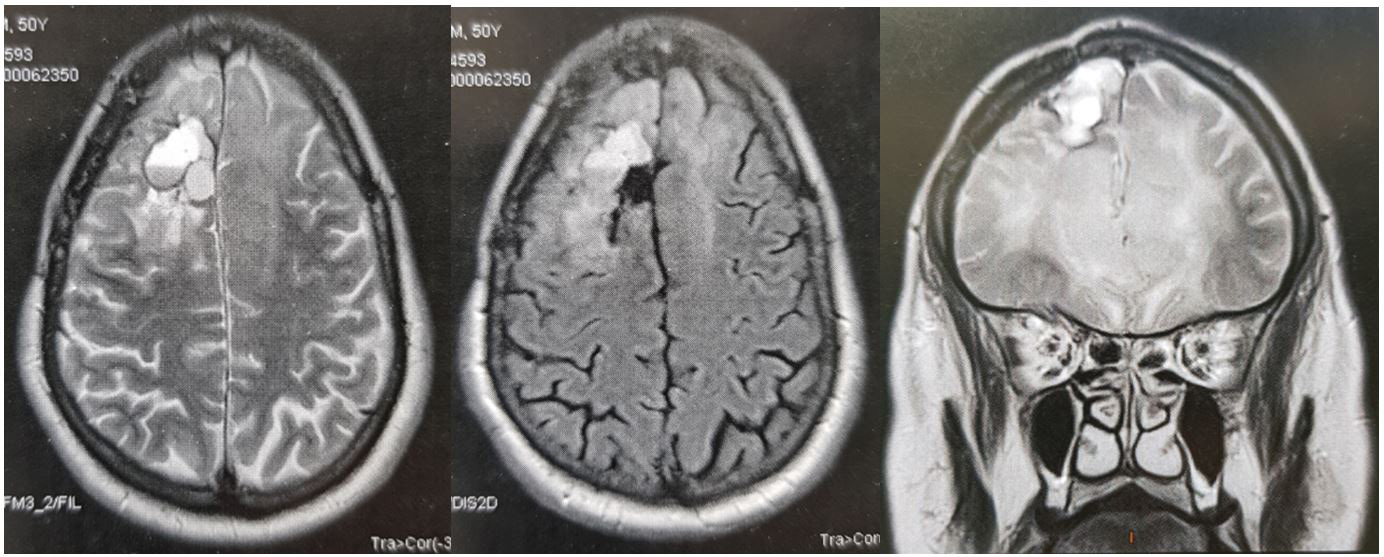 |
Figure 4: T2-FLAIR axial and T2 coronal MRI sequence showing right frontal hypersignal lesion suggesting tumor recurrence |
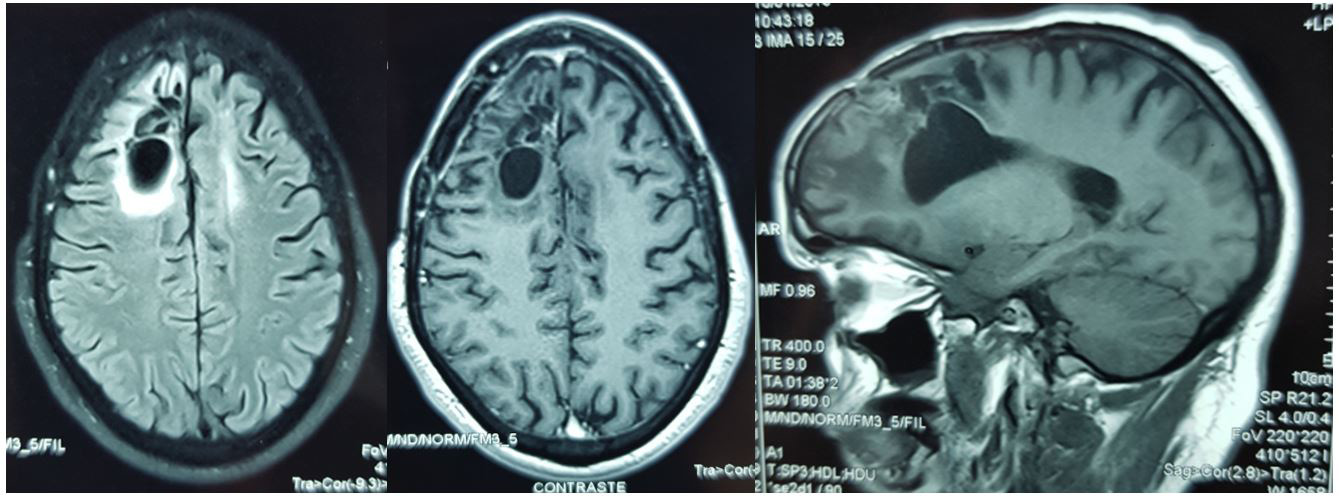 |
Figure 5: T2-Flair axial MRI sequence and T1-weighted axial and sagittal gadolinium-enhanced MRI without enhancement and tumor residue |




































