Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2019 Ardhaoui H. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Cystadenolymphoma of the parotid gland is synonymous for papillary cyst adenoma lymphomatosum (PCL) or warthin’s tumor. It is the most common benign tumor of the parotid gland after pleomorphic adenoma, with a rare possibility of malignant transformation. It manifests as a slow growing fluctuant mass, due to its cystic morphology. The treatment of choice is complete excision. We report a 60 year old male patient with a huge parotid tumor of two years evolution, which turned to be a cystadenolymphoma on histopathology
Keywords:Cystadenolymphoma; Parotid; Giant; Warthin’s tumor
Warthin’s tumor is a benign salivary gland tumor accounting for up to 17% of all salivary gland tumors [1]. It affects mostly the parotid gland of middle aged patients, with more men suffering from it than women at a sex ratio of 5:1 [2]. It can be multifocal in 12% of cases while bilateral lesion occurs in only 6% of patients [3]. These tumors are 8 times more frequent among smokers, although the exact pathogenesis is still unknown [4].
The size can be few millimeters to centimeters, with an average of 2 to 4 cm [5]. Diagnosis is usually based on ultrasonography combined with a computed tomography or magnetic resonance imaging scan, though it requires histological confirmation [6]. Optimal treatment of warthin's tumors is still controversial, yet general consensus requires surgical removal with uninvolved margins.
This report describes the successful excision of an enormous warthin’s tumor of the parotid gland, with its clinical, radiological features and shows surgical challenge faced.
It is a case study
A 60 year old male patient was admitted to the ENT department for an enormous mass of the left parotid. On admission, he was complaining of swelling in his neck. The swelling was so large that it affects his quality of life. It was insidious in onset, gradually increasing of size over the past two years. He had no other associated signs in particular no discomfort while swallowing nor breathing difficulty. He has no history of weight or appetite loss. His medical history revealed that he had been smoking 20 cigarettes a day for 40 years.
Physical examination shows on inspection, a huge swelling in the left side of neck. The skin over the swelling was normal, stretched and had no inflammatory sign. The palpation reveals a solid mass measuring about 13 cm in the left parotid area, non-pulsatile, non-reducible and freely mobile with no attachment to underlying structures, with no cervical lymph nodes. Intraoral examination doesn’t reveal any abnormalities (Figure 1).
MRI was prescribed, and has shown voluminous pseudo-cystic lesions occupying the left parotid lobe with left exophytic laterocervical development and a small deep component. The lesion measures 115 * 90 * 70 mm. Its signal was pseudo liquid hyper intense in T2 and hypo intense in T1. Right parotid was normal in appearance with no cervical lymphadenopathy (Figure 2).
The patient underwent to surgical excision of the tumor under general anesthesia after consent. A modified Blair’s incision was performed, followed by tissue dissection to expose the parotid gland. The main trunk of facial nerve was identified, and the branch was dissected. Dissection was carried on carefully respecting neurovascular structures, and the tumor was removed completely. The intervention was concluded with surgical drains placement and skin suturing. Excised mass was sent to the pathology department and has revealed the diagnosis of Warthin’s tumor.
No complications were recorded in the postoperative period in particular no facial nerve palsy. The patient was discharged 3 days after the surgery (Figure 4).
Warthin’s tumors are considered to be the second most frequent type of salivary glands tumors after pleomorphic adenomas, accounting for 6 to 10% [4]. It actually has several different names referring to its histological features, including: papillary cyst adenoma lymphomatosum, cystadenolymphoma or adenolymphoma. Warthin’s tumor term is the preferred one, widely used to avoid confusion with malignant lymphoid neoplasm [7].
It can be diagnosed at any age, but predominantly arises in the 6th and 7th decade in male population, with rare cases below 40 years of age. Long ago, male to female ratio was approximately 5:1. However, nowadays recent studies has shown increasing incidence among female sex, reducing the sex ratio to an almost equal rapport [8]. This can be explained by the spreading smoking habit among women. It has been described that Warthin’s tumor is 8 times more frequent among smokers than non-smokers, with more than 90% of tumor patients having a history of smoking; hence showing clear correlation between smoking and the occurrence of the tumor [9].
Clinically, Warthin’s tumor doesn’t grow aggressively. It appears as a round or an oval shaped slow growing and painless swelling of the parotid region. However, sometimes patients may complain of tinnitus, little pain, otalgia or deafness. It is almost exclusively located in the superficial parotid gland with a high predilection for the tail lobe, rarely the deep one.
The size can vary between several millimeters to centimeters, with an average size at diagnosis of 36 millimeters of the diameter. According to a study, 56% of a total of 278 subjects had 1-3 cm, 40% 4-6 cm, and only one patient having over than 10cm [2]. Though, huge Warthin’s tumor as in this report measuring clinically up to 13 cm couldn’t be described in literature.
Ultrasound of the parotid gland and local lymph nodes is usually used in the first lane, but seems to be limited. Therefore, it is often combined with other radiological examinations. CT scan and MRI allow accurate assessment with a specificity and sensibility of 91% for the MRI [10]. Scintigraphy with radioisotope T99m Pertechnetate is often helpful in the diagnosis of parotid gland tumors because the Warthin’s tumor captures the isotope and behaves like a hot spot [11]. Recently, a new diagnostic tool has been described. It is fine needle aspiration cytology (FNAC) showing a sensitivity of 90.4% and a positive predictive value (PPV) of 98.1% [12].
Although the clinical and radiological features of the parotid mass allow an assessment prior to surgery, confirmation is obtained only by the histo pathological study.
In fact, there are several conflicting opinions about warthin's tumors treatment [13]. It is still controversial. General consensus requires surgical removal with a wide tumor free margin to prevent potential recurrence or malignant transformation [6]. Thus, it is important to bear in mind that warthin’s tumors can be bilateral between 5 to 10% of cases, can degenerate in 0.3%, and reoffend after local excision in 1.8%. Therefore, large excision with uninvolved margins is highly recommended [11].
Other than the huge size of the tumor as the case described above, the location of the mass in the deep lobe of the parotid gland is a real dilemma of a suitable approach; making total parotidectomy the only substantial alternative [4].
Post operative complications are rare and usually limited to: hematoma, temporary paralysis of the facial nerve and Frey’s syndrome. However, some authors showed that the nerve damage was related to the size of the tumor. They indicated that tumor lengths equal or exceed 3 cm had a significant higher risk of facial nerve injury [14]; a challenge that has been took up in our case.
PCL or Whartin’s tumor is a benign salivary gland tumor with a large spectrum of symptoms from a small discomfort to a large and deforming swelling. Definitive diagnosis requires histological confirmation. The treatment of choice is based on careful surgical excision, respecting the neurovascular structures especially the facial nerve. Surgery with tumor free margins in order to prevent recurrence or possible malignant transformation.

![]()

 |
Figure 1: Preoperative findings: mass of the left parotid gland |
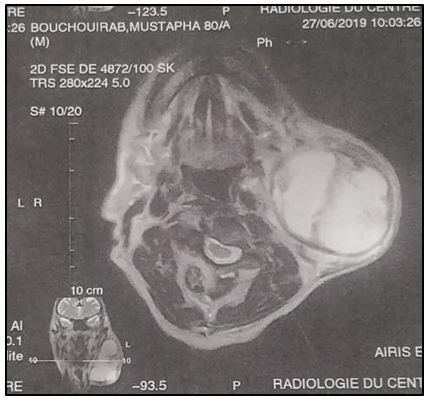 |
Figure 2: Preoperative MRI findings: axial view |
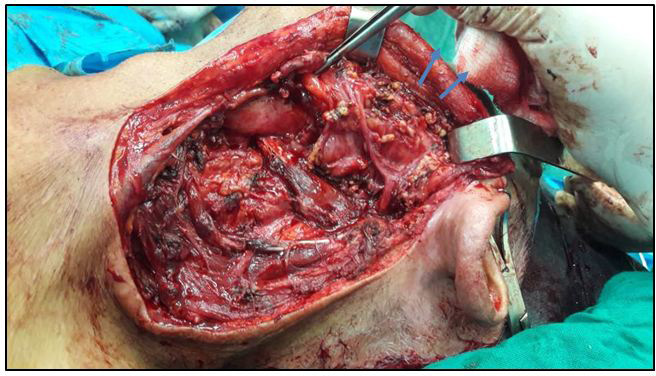 |
Figure 3: Intra operative picture after excision of the tumor respecting the facial nerve and its ramifications which are intact (arrows) |
 |
Figure 4: Warthin’s tumor after complete resection |




































