Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2019 Raksha K. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Universal and routine access to quality assured HIV related laboratory services has been the goal of all national programs concerned with HIV infection in India. Although guidelines for Prevention of Parent to Child Transmission [PPTCT] with regards to testing strategies and initiation of antiretroviral therapy [ART] are made available, the management of 'indeterminate' cases during pregnancy for both the mother and the neonate poses a clinical dilemma and a diagnostic challenge. In this report, we describe a pregnant patient of indeterminate HIV status who delivered a baby through emergency Caesarean section due to intrahepatic cholestasis of pregnancy and an impending HELLP Syndrome, also the diagnostic and therapeutic issues we faced during their management. We have also discussed the pros and cons of the current recommended guidelines and the lacunae that can be filled for better HIV diagnosis and treatment in this modern era of medical advancements to prevent perinatal transmission.
Keywords:HIV in Pregnancy; Indeterminate Status; Perinatal Transmission; NACO Guidelines
List of abbreviations: ANC: Antenatal Checkup; APGAR: Appearance Pulse Grimace Activity and Respiration; ART: Antiretroviral Therapy; CDC: Centers for Disease Control and Prevention; CMIA: Chemiluminescent Microparticle Immunoassay; ECLIA: Electrochemiluminescence Immunoassay; HELLP: Hemolysis Elevated Liver Enzymes and Low Platelet Count; HIV: Human Immunodeficiency Virus; ICTC: Integrated Counselling and Testing Centres; IFA: Immunofluorescent Assay; LSCS: Lower Segment Caesarean Section; NA: Not Applicable; NACO: National Aids Control Organization; NACP: National AIDS Control Programme; NICU: Neonatal Intensive Care Unit; NNRTI: Nonnucleoside Reverse Transcriptase Inhibitor; NR: Not Reported; NRHM: National Rural Health Mission; NRL: National Reference Laboratory; OD: Optical Density; PPTC: Prevention of Parent to Child Transmission; PCR: Polymerase Chain Reaction; RDT: Rapid Diagnostic Test; sdNVP: single dose Nevirapine; SRL: State Reference Laboratory; WB: Western Blot; WHO: World Health Organization
Mother-to-child-transmission of HIV is a major route of HIV infection in children. Perinatal transmission can occur during pregnancy [intrauterine], during labour and delivery [intrapartum], or after delivery through breast- feeding [postpartum]. In the absence of breast-feeding, intrauterine transmission accounts for 25-40% of infection, and 60-75% of transmission occurs during labour and delivery [1].
A joint directive by the National AIDS Control Programme [NACP] and the National Rural Health Mission [NRHM] was issued in July 2010, explicitly stating that universal HIV screening should be included as an integral component of routine Antenatal check-up [ANC]. The objective was to ensure that pregnant women who are diagnosed with HIV would be linked to HIV services under the Prevention of Parent to Child Transmission [PPTCT] programme. HIV Testing is thus simplified and made an important component of routine perinatal care [2].
Recommended guidelines follow a voluntary approach to HIV testing [3].The strategy is the cornerstone of HIV diagnosis and is based on serial testing. The type of strategy adopted depends on the ultimate purpose of HIV testing. An essential prerequisite for the use of the algorithm is that the first, second, and third tests [A1, A2 and A3] employed are based on different serological principles and/or use of different HIV antigens in the assay [4].
False positive HIV results though uncommon in pregnancy, they are a known phenomenon especially in multiple pregnancies [4]. However, in India there is little guidance for the immediate management of ‘Indeterminate’ results in pregnant patients and additional testing strategies with prophylaxis guidelines for the newborn. We describe a case of ‘Indeterminate’ HIV test result during pregnancy and delivery and the issues we faced in the management of the patients-the mother and the neonate.
A 29-year-old pregnant woman present to our obstetrics department in May 2019 at 33 weeks of gestation with history of itching in palms and soles for one week. She reported no other major health concerns. Her vitals were stable and other physical examination findings were within normal limits. Her liver function tests were monitored and found to be deranged and platelet counts were on the lower side of the normal range. Ursodeoxycholic acid 300 mg twice a day was started. Viral markers for hepatitis were negative. Her ultrasound abdomen showed normal findings. Written informed consent was taken with pre-test counselling before the test for HIV as per the hospital protocol.
HIV Combi PT Assay by Electrochemiluminescence[A1] showed Reactive with an Optical Density [OD] value of 1.87[Cut off-1.00], a repeat sample was collected as per protocol and HIV 1 & 2 ELISA [A2] was done which was also found to be Reactive with an OD value of 1.618 [Cut off-0.213]. HIV 1 & 2 Chemiluminescence [A3] was Non-reactive with OD value of 0.48[Cut off -1.00]. HIV Tridot and additional serological tests were done which were Nonreactive (Table 1).
When the provisional report was communicated to the treating obstetrician, upon eliciting history it was found that there were no factors contributing to the acquisition of HIV infection. No blood transfusion, needle stick injury, exposure through high risk behaviour. The husband’s history, clinical examination and HIV Combi PT Assay by Electrochemiluminescence were Nonreactive. As per Strategy 3 of NACO guidelines (Figure 1), the result was considered as ‘Indeterminate’ and the same was communicated to the couple along with post-test counselling. Meanwhile, her liver enzymes were showing derangement and emergency Lower Segment Caesarean Section [LSCS] had to be conducted in view of cholestasis of pregnancy. A female baby weighing 1.62 kg/3.6 lb (Percentile 0.1%, Z score- -3.7) with low birth weight was delivered. Baby was alive, cried after suction and stimulation. APGAR score was 7/10 at 1 minute and 8/10 at 5 minutes. The baby was admitted in the Neonatal Intensive Care Unit [NICU] in view of prematurity, respiratory distress and feed intolerance. General physician and infectious disease specialist consultation was sought during the delivery for the ‘indeterminate’ HIV status of the mother and decision to administer the first dose of Nevirapine syrup to the baby was made..
Meanwhile given the conflicting serological results of the mother, her HIV-1 viral load by Real Time PCR was done by HIV-1 Quant Assay, performed on GeneXpert® Instrument Systems, designed for the rapid quantitation of Human Immunodeficiency Virus type 1 (HIV-1) in human plasma from HIV-1 infected individuals over the range of 40 to 10,000,000 copies/mL. The test results showed ‘HIV-1 Not Detected’. This test however does not detect HIV-2 RNA (Qualitative RNA) and Quantification (Viral Load). Her CD4 Count was 654 cells/mcL [Normal range for females-449-1372 cells/mcL].
A repeat Chemiluminescent microparticle immunoassay (CMIA) done in an outside laboratory on a third sample for interlaboratory comparison was found to be Nonreactive. Upon receipt of the same, both the partners were counselled regarding all the test reports and the occurrences of false positives in pregnancy. HIV-1 Proviral DNA Detector for the neonate was advised but was not tested in view of the negative viral load report of the mother and this was considered as a serological false positive. Repeat assays on follow up were not performed for parents and neonate in view of the same.
Importance of Sequential Testing
The WHO guidelines on HIV Testing Services [HTS] focus on the 5 C’s: Consent, Confidentiality, Counselling, Correct Results and Connection. The rationale behind the sequential positive Rapid Diagnostic Tests [RDT] to confirm HIV diagnosis when performed correctly is that the multiplicative effect of combining highly specific RDTs should reduce the misdiagnosis [5].
As per Strategy 3 (Figure 1) of National Guidelines for HIV Testing-National AIDS Control Organization to detect HIV infection in asymptomatic individuals [ICTC’s, PPTCTC’s] three assays are used in pregnant patients. Assays A1, A2, A3 represent 3 different assays based on different principles or different antigenic compositions. Assay A1 should be of high sensitivity and A2 and A3 should be of high specificity. A2 & A3 should also be able to differentiate between HIV 1 & 2 infections [4].
In case the results are indeterminate, testing should be repeated on a second specimen taken after 14-28 days. In case the serological results continue to be indeterminate, then the specimen is to be subjected to a Western Blot/Polymerase Chain Reaction [WB/PCR] if facilities are available or refer to the State/National Reference Laboratory [SRL/NRL] for further testing. Samples with indeterminate results are to be sent to SRLs/NRLs for confirmation [e.g., Western Blot]. Results obtained are then to be communicated to the individual. The follow-up specimen from patients with indeterminate result should be collected two weeks after the first specimen collection. However, if the confirmatory test fails to resolve the serodiagnosis, follow up testing should be undertaken at four weeks, three months, six months, and 12 months. After 12 months, such indeterminate results should be considered negative. However, the molecular assays [HIV-1 and HIV-2 NAT] can be used to resolve specimens repeatedly [>2 times] giving indeterminate results [4].
In a resource limited setting, Rapid Diagnostic Tests [RDTs] are the primary diagnostic tools for diagnosis of HIV, also the quality of RDTs is highly dependent on user training and quality assurance of the diagnostic laboratory. There is concern of false positive [FP] RDTs which could lead to misdiagnosis of HIV infection and inappropriate ART if recommended algorithms are not followed. Testing centres for HIV are often burdened with high workload and lack of training and compliance to quality assurance [5].
In a retrospective study done by Hsiao et al in a cohort of pregnant women attending antenatal services at a public sector primary care facility in Cape Town, South Africa, between 2013 and 2014, 3/952[0.3 %] HIV RDT diagnoses were found to be false positive. The testing algorithm was based on the World Health Organization’s [WHO]-recommended two test strategies, two third-generation HIV antibody RDTs was used for confirmation. The study also found that compared to the cost of confirming the RDT based diagnoses, the cost of misdiagnosis of HIV is high with erroneous initiation of ART, lifetime of anti retrovirals and viral load monitoring for one person [5]. Enzyme Immunoassays [EIA] used in RDTs is highly sensitive and specific, but there is a perception that pregnant women are at higher risk for false-positive results. If this perception is shared by clinicians, they may be less likely to adopt universal screening [6].
The cross reactivity between viral proteins and tested specimens causes the false positive HIV antibody test results, but such cross reactivity is less common in peptide based EIAs which contain fewer antigens than previous viral lysate based EIAs. When compared to Western Blot, the new EIA can detect infections earlier hence the role of Western Blot for confirmation in such indeterminate cases is obsolete [6].
In a PrEP Implementation for Mothers in Antenatal Care [PrIMA] study done by Wagner et al in Kenyatta National Hospital, University of Washington, Kenya involving cluster RCT of approaches for integrating PrEP into antenatal care in western Kenya between January to November 2018 among 3,031 women, 6,182 HIV retest sessions conducted, 8 discrepant rapid results [0.13%, 95% CI: 0.06-0.25%] among 6 women. 5 women not using PrEP at time of testing; 1initiated PrEP but reported poor adherence and had not taken PrEP within 14 days prior to HIV test. At later visits, 2 women had recurrent discrepant rapid results with negative PCRs when retested; one had concordant positive rapid results at delivery; she initiated ART and had two negative PCRs and negative ELISA [7]. Each testing situation is different, and not all testing strategies are appropriate for all testing situations. Obtaining testing after several weeks after an initial indeterminate result is impractical for pregnant women who are due for delivery. False positive results can cause serious emotional distress and unnecessary follow up and hence should be handled delicately by appropriately trained physicians and counsellors. Guidelines or testing algorithms are necessary for special situations of indeterminate results in cases like pregnancy and delivery to aid in peripartal diagnosis and treatment when the risk of transmission is high and can be avoided. Without a proper confirmation algorithm, there is concern of either over diagnosis and unnecessary treatment for a false positive result or under diagnosis and impending HIV perinatal transmission for a false negative result.
Also, in indeterminate status of the mother, the prophylactic management of the neonate becomes a cause of concern. In our patient weighing the benefit more than the risk, single dose Nevirapine [sd-NVP] was administered to the neonate while the HIV-1 viral load and CD4 count of the mother was awaited. The use of single dose Nevirapine [sd-NVP] at the onset of labour significantly reduces peri-partum HIV transmission. However, this approach is less effective than other antiretroviral prophylactic regimen and may be associated with acquisition of viral resistance to non-nucleoside reverse transcriptase inhibitor [NNRTI] drugs. Additionally, the use of sd-NVP does not reduce HIV transmission risk during the breastfeeding period as per evidence [2]. The updated guidelines
The Centre for Disease Control and Prevention [CDC] in 2014 changed its diagnostic algorithm to include nucleic acid amplification testing for those samples found to be indeterminate using HIV immunoassays. CDC recommends testing with a combination immunoassay that detects HIV-1 and HIV-2 antibodies and HIV-1 p24 antigen. All specimens reactive on this initial assay are to undergo supplemental testing with an immunoassay that differentiates HIV-1 from HIV-2 antibodies. Specimens that are reactive on the initial immunoassay and nonreactive or indeterminate on the antibody differentiation assay proceed to HIV-1 nucleic acid testing for resolution [8].
CDC no longer recommends HIV-1 Western blot and HIV-1 IFA, previously recommended to make a laboratory diagnosis of HIV- 1 infection, Positive results from the recommended algorithm indicate the need for HIV medical care and an initial evaluation that includes additional laboratory tests [such as HIV-1 viral load, CD4+ T lymphocyte determination, and an antiretroviral resistance assay] to confirm the presence of HIV-1 infection, to stage HIV disease, and to assist in the selection of an initial antiretroviral drug regimen [8]. Elimination of Western Blot as the confirmation test reduces turnaround time and the chance of false negative result. Addition of molecular testing for viral nucleic acid in the algorithm in the initial testing phase addresses the issue of false positives and confirm acute HIV infection [9].
A retesting policy in low prevalence populations like pregnant women that does not delay ART initiation to the neonate is therefore necessary in our national guidelines. This will benefit the pregnant women in a timely way before the onset of labour and avoid undue stress on someone who is not infected.
In an era of major scientific advances to reduce perinatal transmission, indeterminate cases during delivery are a great challenge for the diagnostician, obstetrician and pediatrician. An updated guideline could be lifesaving and cost saving.
No diagnostic test or algorithm can be completely accurate in all cases of HIV infection, inconsistent or conflicting test results obtained during the clinical evaluation warrants additional testing of follow-up specimens based on strong evidences and recommendations. The physical, emotional and social aspects of the patient and the family per se are to be considered in our algorithms. Testing algorithms and national programmes therefore should strive for constant quality improvement and strengthen the HIV diagnostics.

![]()

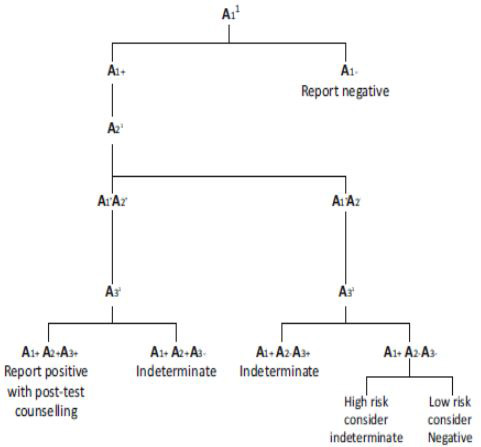 |
Figure 1: Strategy 3 to detect HIV infection in asymptomatic individuals [ICTC’s, PPTCTC’s] |
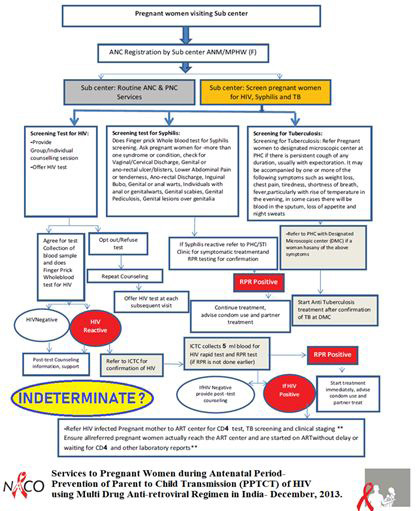 |
Figure 2: Services to Pregnant Women during Antenatal Period, as per Updated Guidelines for Prevention of Parent to Child Transmission [PPTCT] of HIV using Multi Drug Anti-retroviral Regimen in India. National Guidelines for Prevention of Parent- to-Child Transmission of HIV. Ministry of Health & Family Welfare. Department of AIDS Control. Basic Services Division,2013 [2] |
Sample |
Test |
Methodology |
Signal/cut-off [S/CO] value |
Cut off index value |
Report |
Primary (1st)sample |
HIV ECLIA*[Elecsys HIV combi PT] |
Electrochemiluminescence |
1.87 |
1.00 |
REACTIVE |
Repeat (2nd)sample |
HIV ELISA [4th generation] |
Enzyme linked immunosorbent assay |
1.260 |
0.213 |
REACTIVE |
Primary (1st)sample |
HIV CLIA** |
Enzyme linked immunosorbent assay |
0.43 |
1.00 |
NONREACTIVE |
Repeat (2nd)sample- 1st run |
HIV ECLIA [Elecsys HIV combi PT] |
Electrochemiluminescence |
2.12 |
1.00 |
REACTIVE |
Repeat (2nd)sample- 2nd run |
HIV ECLIA [Elecsys HIV combi PT] |
Electrochemiluminescence |
2.01 |
1.00 |
REACTIVE |
Primary (1st)sample |
HIV TRIDOT |
Immunochromatography |
NA** |
NA** |
NONREACTIVE |
Outside laboratory 3rd sample |
HIV 1 & 2[P24 ANTIGEN & ANTI- BODY DETECTION] [CMIA] |
Chemiluminescent microparticle immunoassay |
NR*** |
NR*** |
NONREACTIVE |
*ECLIA- Immunoassay for the in vitro qualitative determination of HIV-1 p24 antigen and antibodies to HIV-1, including group O, and HIV-2 in human serum and plasma. **CLIA-Immunometric assay using 4 recombinant antigens (HIV-1 Env 13, HIV-1 Env 10, HIV-1 p24, and HIV-2 Env AL) derived from HIV-1 core, HIV-1 envelope and HIV-2 envelope, CMIA- Chemiluminescent microparticle immunoassay **NA: Not Applicable; ***NR: Not Reported
Table 1: Serial testing as per NACO guidelines, values and interpretation




































