Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2019 Bilge H. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Objective: Intramural hematoma is a rare complication of oral anticoagulant therapy that occurs in 0.04% of patients treated with warfarin. In this article, we present this case to raise awareness about the diagnosis and management of this disease.
Case presentation: We present a 79-year-old woman who presented with abdominal pain for 2 days. The patient, who received anticoagulant therapy with warfarin for 4 years, had an INR value of 14.82. Intramural small bowel hematoma was revealed through abdominal CT scan. The patient with abdominal pain and abdominal distension was treated succesfully with conservative fluid resuscitation, pain control, INR monitoring and bowel rest.
Conclusion: Abdominal complaints and high INR indicate a possible diagnosis of intramural small bowel hematoma, but these abdominal symptoms may range from mild pain to an established acute abdomen. A CT scan demonstrating symmetrical bowel thickening associated with some luminal constriction confirms the diagnosis. In terms of management, there is insufficient evidence to support a standard treatment; Still, the most accepted approach seems to be conservative treatment after exclusion of complications requiring surgical intervention.
Keywords:Warfarin; Spontaneous Intramural Hematoma; Close follow-up; treatment
Spontaneous small bowel hematoma was first described in 1838 [1]. Intestinal intramural hematoma is most commonly seen in the duodenum, especially in childhood, whereas spontaneous intramural hematoma is most commonly seen in the jejunum [2]. Bleeding as an intramural hematoma of the small bowel is rare, with a rate of 0.04% [3]. If the diagnosis can be confirmed, conservative treatment is usually achieved by correcting coagulation parameters [4]. Computed tomography (CT) is the most commonly used imaging modality in diagnosis[ 5]. Hematoma; most commonly seen in jejunum (69%), ileum (38%) and duodenum (23%) 5].
In this study, we present a case of non-traumatic small intestine followed by conservative approach in our clinic with the diagnosis of intramural hematoma and current approaches of treatments have been emphasized.
A 79-year-old female patient presented to the emergency department with pain, swelling and bruising in the right upper quadrant for 2 days. She had been receiving Warfarin 5 mg (Coumadin 5 Mg 28 Tablets, Zentiva Health Products Industry and Trade Inc.) for 4 years for atrial fibrillation. However, the relatives of the patient forget that she has recently taken the drug and she has taken additional doses daily. She had a history of type 2 DM, hypertension, heart valve disease, and chronic atrial fibrillation. Recently, dementia symptoms have started to appear in the patient. The patient had bruising and pain at the injection site as a result of an injection into the right upper quadrant. There was no other history of trauma. Her blood pressure was 175/95 mmHg, and her pulse was 78/minute.
Physical examination revealed an ecchymotic region of approximately 20 cm in the right upper quadrant and a painful, hard lesion of 5-6 cm. All the abdominal dials had sensitivity. Intestinal sounds were hypoactive.
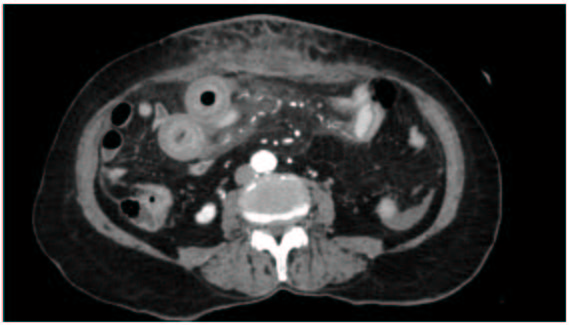
Laboratory data; INR value was 14.82, hemoglobin was 8.0 g / dL and hematocrit was 25.7. Previous INR values could not be reached because the patient was followed-up in another center. Superficial tissue ultrasonography showed an appearance consistent with approximately 5 cm rectum hematoma. Abdominal tomography showed edematous thickening of the intestinal ans wall in the paraumbilical region of the abdomen and appearance consistent with intramural hematoma (Figure 1).
Oral intake was discontinued. She was admitted to the general intensive care unit for intravenous hydration, pain control and conservative treatment. Here, Warfarin was discontinued and enoxaparin sodium (Clexane 40 MG Injection, Sanofi India Ltd.) was started with the patient who was followed together with the anesthesiologists. Fresh frozen plasma was given twice a day, the INR value fell to normal limits. On the 3rd day of follow-up, the patient's abdominal findings regressed and discharged. The patient who tolerated enteral nutrition was taken to the ward. The patient was discharged on the 7th day of follow-up. After 15 days, the patient did not have any complaints. Laboratory findings were normal.
Intestinal intramural hematoma was first described by Mc Lauchlan in 1838 (1 Nontraumatic intestinal intramural hematoma is a rare complication of anticoagulant therapy and small bowel obstruction caused by intramural hematoma is a rare condition [6,7].
Pathophysiology; It occurs when the terminal artery originating from the mesentery and feeding the muscle layer of the intestinal wall is ruptured and hemorrhage accumulates between the muscularis mucosa and intestinal muscle layers [5,8]. Hematoma rupture may occur with gastrointestinal bleeding. Hematoma complications such as necrosis, perforation and hemoperitoneum should be suspected in the presence of signs of peritoneal irritation [9].
Typical findings on abdominal tomography are diagnostic, and peripheral wall thickening, lumen narrowing, hyperdensity and obstruction may be seen [5]. Yoldas et al., in a study conducted in 2013, detected CT findings in 71.4% of patients with intestinal intramural hematoma [9]. Abdominal ultrasound can detect intestinal dilatation and segmental edematous changes in the intestinal Wall. In our case, we made the diagnosis with CT. In the differential diagnosis, inflammatory bowel diseases and colon malignancies should be taken into consideration [9].
Due to its rare clinical appearance, there are not enough studies to standardize treatment. Close follow-up by surgeons, anesthesiologists and intensive care providers is critical for the mortality of patients. During treatment, anticoagulant drugs are discontinued first, bleeding parameters are normalized with vitamin K and fresh frozen plasma supplementation. In patients without signs of peritoneal irritation or complications, the clinical picture improves with conservative treatment within 5-7 days [10,11]. Anticoagulant therapy can be resumed after regression of hematoma and clinical recovery of the patient. As in our case, surgical treatment should not be performed in patients without complications.
Abdominal complaints and high INR indicate a possible diagnosis of intramural small bowel hematoma, but these abdominal symptoms may range from mild pain to an established acute abdomen. A CT scan demonstrating symmetrical bowel thickening associated with some luminal constriction confirms the diagnosis. In terms of management, there is insufficient evidence to support a standard treatment; Still, the most accepted approach seems to be conservative treatment after exclusion of complications requiring surgical intervention.
This case report had no involvement sponsors.
The authors have no conflict of interests to declare.
This case report is exempt from ethical approval by our institution.
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.

![]()

 |
|




































