Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2019 Borg H. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Thousands of patients are annually diagnosed with Frozen Shoulder (FS) or adhesive capsulitis, where the joint capsule contracts and becomes less flexible. The condition is painful, with reduced range of motion (ROM) in the shoulder and arm and causes great suffering, often with difficulty sleeping and greatly reduced work ability. The treatment given today is partly conventional treatment with cortisone or NSAID preparations as well as physiotherapy and other therapeutic treatment which usually have limited effect. The study investigates whether myofascial treatment, using a device generating deep pulsating vibrations, can provide increased ROM and facilitate for these patients. 23 patients diagnosed with FS were included in the study. Three treatments were performed, within set time intervals. The ROM was measured before and after each treatment, pictures were taken with a thermography camera and angles were measured. The result showed that 87 percent got an increased ROM by 30 degrees or more, that 52 percent of the patients improved ROM by 60 degrees or more, and that 30 percent regained full ROM. 61 percent of the patients also reported improved quality of sleep. The study indicates that this treatment could possibly improve ROM and well-being for patients with FS. Further studies are recommended to evaluate and validate these findings. A validated treatment of FS could mean great socioeconomic benefits and an increased quality of life for patients diagnosed with FS.
Keywords:Frozen Shoulder; Adhesive Capsulitis; Fascia; Myofascial Pain; Fascia Treatment; Myofascial Treatment
Frozen shoulder (FS), adhesive capsulitis, is a common disease characterized by gradual decreased, active and passive movement of the glenohumeral joint. The disease course is a gradual process that starts with inflammation of the synovial fluid and progresses to fibrosis in the joint capsule, which contracts and solidifies, which occurs in four different clinical stages (Hannafin et al, 2000) [1]. FS is divided into primary or secondary FS. Primary FS, also idiopathic FS, occurs spontaneously without any known cause or trauma, while secondary FS is caused by trauma or immobilization of the shoulder (Zuckerman et al, 2011) [2]. The initiator of synovitis in primary FS is unclear but Kanbe et al (2009) [3] found molecules related with mechanical stress in the synovium. The first stage, which lasts a few months, is characterized by inflammatory processes in the synovial fluid, but the joint capsule is intact (Hannafin et al, 2000)[1]. The patient experiences severe pain during certain movements, which results in a reduced range of motion (ROM) but also pain at rest and during the night. This can also cause the patient to avoid moving the arm and more immobility leads in turn to even more stiffness and reduced ROM, (Stecco et al, 2013) [4]. In stage 1, the decrease in ROM appears to be largely due to the pain and not to the joint capsule being densified. There also were more signs of inflammation in stage 1, which begin to decline in stage 2. In the later stages, changes have begun to occur in the joint capsule's connective tissue which has begun to densify, and scar tissue and fibrosis can be seen, and the inflammation is declining. The pain has increased gradually and is more persistent and this can continue for many months up to a year or more. Then the pain begins to decrease but the shoulder becomes more immobile and stiffer, it has "frozen". FS starts to heal and improves slowly, and this stage can continue for a long time, up to two years. However, a certain limitation in the ROM often remains afterwards (Hannafin et al, 2000) [1].
Primary FS, without any obvious preceding cause, is diagnosed by history and physical examination while other causes of motion loss and pain are excluded (Hannafin et al, 2000) [1]. Due to the slow creeping course of primary FS, it is common for the patient not to notice the deterioration in ROM but only to respond to slowly increasing pain in the shoulder (Manske et al, 2008) [5]. FS is most common between the ages of 40 and 60 and affects about three percent of the population and is also more common in women. Also, patients with diabetes are at increased risk of getting the disease (Manske et al, 2008) [5]. The condition is difficult to treat and hitherto, treatments consist of corticosteroids and NSAIDs as well as physiotherapy and home exercises with limited results. It is known that vibration and oscillation stimulate and facilitate circulation and flow in the fascia and release tension (Comeaux, 2010) [6].
The fascia has a variety of functions, including power transmission, movement, stability, proprioceptive communication and by providing a sliding layer and reducing friction in connection with movement (Kumka and Bonar, 2012) [7]. The fascia is abundantly innervated and contains a large number of free nerve endings and proprioceptors (Stecco et al., 2007 [8]; Stecco et al., 2013 [4]; Bhattacharya et al., 2011) 9]. Densification and adhesions in the fascia and its extracellular matrix (ECM) are related to decreased glide ability due to increased viscosity (Stecco et al., 2011, 2013, 2018; Langevin et al., 2011; Chaitow, 2014) [4,1011-13]. Stecco et al suggest that the viscoelasticity of fascia can modify activation of the nervous receptors within fascia. These mechanoreceptors respond to the viscoelasticity in surrounding tissue and if they are overstimulated, they can become nociceptors (Stecco et al, 2007, 2013) [4,8].
Cells in the fascia, specialized in producing hyaluronic acid (HA) for the ECM, like the cells in the subsynovial membrane, have been demonstrated, together with the importance of the role of HA in maintaining the viscoelasticity of a healthy fascia and how this affects a variety of pathological conditions such as myofascial pain, muscle contractures, densification, fibrosis, etc. (Stecco et al., 2011, Stecco et al., 2013; Stecco et al., 2018) [4,10,11]. It has been known in the past that changes in HA concentration are associated with inflammation and degenerative joint diseases (Temple-Wong et al., 2016) [14] and that problems with the facial glide function can interfere with the whole tissue's function and induce pain (Stecco et al, 2013 [4]; Bordoni et al, 2014) [15]. It is also generally known that HA has an active role in the healing processes of the tissue. HA is a high molecular weight polysaccharide and is a key component of the ECM in the loose fascia, including between deep fascia and muscle, within muscles and between the collagen layers in the deep fascia. It is also a major component of articular joint synovial fluid, where it provides the viscoelasticity and lubrication to protect the joint cartilage. HA has a wide variety of physiological functions in the body, including maintenance of a viscoelastic cushion to protect tissues and to facilitate smooth gliding during movement and in transmission of force from muscle contraction, receptor mediated signaling, cell migration, inflammation and healing properties. Thus, HA has a fast turnover rate and it is also known that it behaves like a non-Newtonian fluid at high concentrations and becomes more viscous (Stecco et al, 2014; Cowman et al, 2015) [16-18]. During inflammatory conditions, concentrations of HA is increased, and the molecules are degraded to shorter chains and lower molecular weight. Changes in HA concentration, molecular weight, inflammatory modifications of HA, binding interactions with other macromolecules, temperature and pH with more, affect the viscoelastic properties of HA and can have dramatic effects on the sliding properties of the fascia. The higher the concentration, the higher the viscosity. (Cowman et al, 2015) [18].
Immobilization of a body segment (as with pain caused by FS) can lead to an increase in the concentration of HA within and between the epimysial fasciae and thus increase the fluid viscosity which in turn decrease the fascial gliding between the layers and give cause for stiffness (Okita et al, 2004; Stecco et al, 2013) [4,19]. Reduced ROM can also give rise to shortening of sarcomere length in muscle fibers in the early stage of immobilization. These changes can increase the number of cross bridges attached during contraction and after several weeks of immobilization the collagen fibrils arrangement in the endomysium adapts and become more circumferential instead of longitudinal to the axis of the muscle fibers (Okita et al, 2004; Cowman et al, 2015) [18,19].
In conditions of inflammation, the concentration of HA increases and the HA-chains begin to entangle into complex arrays and altering the viscoelastic properties that can give rise to myofascial pain. Then, the HA becomes adhesive rather than lubricating, and the distribution of ROM in lines of force, within the fascia become altered. By increased viscosity, the receptors within the fascia can get over-stimulated and send a pain message from a degree of stretching of the fascia that is even within the physiological range (Stecco et al, 2007, 2013) [4,8. ]When concentration of HA is altered, it triggers a cascade of changes, leading to fibrosis due to the deposition of collagen within and between muscle bundles. This in turn leads to further increase in ECM viscosity in the surrounding tissue and restarting the circle (Stecco et al, 2013 ; Stecco et al, 2014)[4,16,17].
The study investigates whether myofascial treatment around the shoulder and myofascial chains (Myers T W, 2013) [20], (in and between muscles, around tendons, joint capsules), using a device generating deep pulsating vibrations, can provide increased ROM and reduced pain for patients with diagnosed primary FS.
The effect of treatment using devices generating deep pulsating vibrations has been tested clinically on horses where changes in muscle tone were measured by multifrequency bioimpedance analysis (Harrisson et al, 2015)[21]. The effect of a similar treatment procedure applied to the shoulders has been studied by Bhagwat, (2010) [22].
Patients
The selection of patients was made using online advertising. The inclusion criteria were a) patients diagnosed with primary FS and b) patients willing to participate in the study. Exclusion criteria included patients who suffered from trauma such as bone fractures, ligation in the shoulder or whiplash injury over the past six months as well as those who have performed arthrodesis, who were pregnant, had implanted prosthesis or suffered from severe osteoporosis.
52 patients applied for the study. 12 were excluded for meeting the exclusion criteria. 23 patients with FS were randomly selected. The 23 spots were made available via an online booking system and the 40 remaining applicants were invited by email. The first 23 patients signing up were called within two days to verify their diagnosis. The study was designed with three sets of three treatment sessions. The first set had five spots and the second and third had nine spots each. At the first session the patients were given written and oral information regarding the study, including background, purpose, study design, consequences and data processing. The patients gave a written consent that they had received the information as well accepting the terms and conditions of the study stating that the study was voluntary meaning they could choose to drop out at any given time, they were to receive no compensation other than the treatment itself and that they were not to undergo any other treatments during the study period.
Of the 23 patients who started the study, 17 completed all three treatments. Three patients interrupted and dropped off the study after the first treatment and two patients dropped off after the second treatment. One regained full ROM after the first treatment and decided not to continue, three patients cancelled for personal reasons and two patients excluded themselves from the study by getting other treatment in between the sessions. The gender distribution was 15 women and 8 men in the age range 27 - 89 years. The duration of symptoms was from two months to two years.
The study was approved by the Swedish Ethical Review Authority in the spring of 2018.
Equipments
The devices used in the study to generate deep pulsating vibrations were Atlasbalans M1 and Atlasbalans M2. These devices provide mechanical vibrations at a variable frequency between 400 to 1200 pulsations per minute in a sine wave. Thermography camera FLIR T540 is used for documentation of ROM. A thermography camera was chosen to keep the patient's images anonymous. ROM was measured using a protractor with 170-180° assessed as full ROM with the arm straight up.
Arrangement
The treatment included three treatment sessions. Treatment one and two were performed with 7 days intervals and the third treatment 37 days after the first treatment. Before the first treatment the patients were asked when and how the symptoms appeared. Before the second and third treatment the patients were asked about what they had experienced since the last session. Before each session, patients were also asked about their experience of perceived pain and their quality of sleep. No pain scales were used to measure the answers.
Photographing
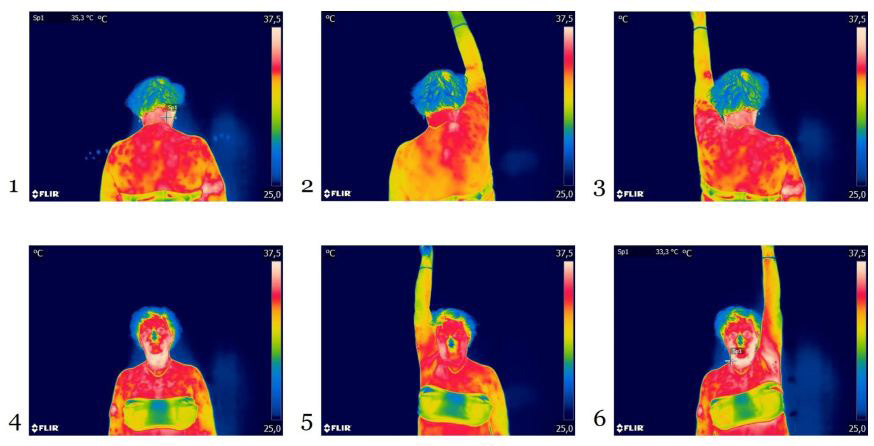
At each occasion, the movement of the arms was measured after a specific pattern, items 1-6 and images 1-6. The movements were performed with both right and left arm regardless of side with dysfunction. The same movements were performed before treatment and after treatment. The ROM was documented with a thermography camera, twelve images of the upper body at each occasion. Images were taken in six different positions, six before and six after treatment item 1-6. The thermography images make the patient anonymous and at the same time they can give an indication of inflammation (high heat) or poor circulation (abnormally cold). In order to repeat the measurements in the same way, all images were taken from the same distance (200 cm), height (150 cm) and from the same angle (90 degrees from the floor). Photography takes place with the patient standing against a light-colored background on a mat with markings where the patient should set their feet. This is to ensure that the patient always has the same starting position. The following angles were imaged in the following order (Item 1-6). This shows a patient with full ROM, 170-180°. Angels were measured with a digital protractor placed on the images.
Patients
1. Back to the camera, arms loosely hanging straight down. 2. Back to the camera, right arm is stretched straight up in abduction. 3. Back to the camera, left arm is stretched straight up in abduction. 4. Face to the camera, arms loosely hanging straight down. 5. Face to the camera, right arm is stretched straight up in abduction. 6. Face to the camera, left arm is stretched straight up in abduction.
Treatment
The treatment is a soft and deep massage treatment. Treatment of the neck, upper back and arm was performed with two devices for about 40 minutes. The following areas were treated.
1. M. Supraspinatus towards the shoulder joint. 2. All muscles between scapula and thoracic spine, M.Levator scapula, M.Serratus, M.Splenius, M.Rhomboideus, M.Trapezius thoracis. 3. Scapula's lower part, M.Infraspinatus, also M.Triceps brachii’s origin at the shoulder joint. 4. Skull base and the neck side and the whole M.Trapezius cervicis towards the shoulder joint. 5. Lateral side of the upper arm, M.Deltoideus and all muscle attachments to deltoid tuberosity of humerus. 6. The lower part of the thoracic spine, the lower part of M.Trapezius thoracis and under the scapula to reach the M. subscapularis, with the arm behind the back. 7. M.Biceps brachii’s long tendon, bursa intertubercularis and M.Pectoralis attachment to shoulder and upper arm. 8. M.Biceps brachii. 9. M. Pectoralis major and minor 10. M. Subclavius
Of 23 patients who started the study, 17 completed all three treatments. Three discontinued after the first treatment (one regained full ROM after one treatment) and three terminated after treatment number two. Of the 17 who completed, seven regained full ROM. All patients were given increased ROM to varying degrees. 61 percent of total 23 patients experienced an improved quality of sleep. Two of the patients who regained full ROM have had the problems between one to two years. The concentration of heat in the neck noted on three patients, disappeared in all cases after the first treatment. Six patients had limited improvement after the treatment (See (Table 1), Patient ID FS01, FS03, FS8, FS10, FS11 & FS20), and all of them have other issues correlated to fascia adhesions (Table 2 and 3).
The study shows positive results for myofascial treatment, using a device generating deep pulsating vibrations, as an alternative for the participating patients diagnosed with Frozen Shoulder (FS). The result shows that the treatment, in a short time, provided increased ROM in the adhesive shoulder and in some cases the ROM was fully recovered. All patients perceived the treatment as pleasant and no patient’s condition got worse after the treatment.
Nine patients regained full ROM and of these, seven were most likely in stage 2 of FS (Hannafin et al, 2000) [1] (one of them regained full ROM after the first treatment and dropped off the study). The other two patients regaining full ROM had had FS between one and two years, stage 3-4, and therefore might have been in a recovery phase, meaning that the treatment could have been speeding up an already existing healing process. In stage 2 of the disease, the inflammatory process in the synovial fluid begins to decrease and instead the connective tissue in the joint capsule begins to densify with increased fibrosis as a result. That could indicate that the treatment affects the flow in connective tissue and reduces the fibrous formation in the joint capsule so that the process turns faster as the inflammation processes have decreased. 61 percent, 14 of total 23 patients, also perceived an improved sleep.
Six of the eight patients that had limited effect of the treatment (less than 60° increased ROM) had other underlying symptoms than FS. Two patients had peritendinitis calcarea, one had had surgery in both knees, two patients had an atrophied deltoideus muscle and one had ceacum appendix surgery ten months prior to the first session. These problems may have had an effect on the results, perhaps due to connective tissue/muscle interactions, abnormal movement pattern, fascia adhesions and so on.
The documentation of the ROM was made with a thermography camera and these images at the same time show that some patients had a clearly increased heat image around the neck-shoulder portion before treatment which disappeared after the first treatment. Inflammation of the tissue gives an elevated heat image and the result indicates that as the flow in the tissue around the painful area improves, this gives a more even temperature in the tissue. There may be a connection between inflammation in the tissue and pain, as well as demonstrated in previous studies (Linnman et al 2011, Hoheisel et al 2015, & Wilke et al 2017) [23-25.]
A major component of the fascia is HA, which affects the density in the fascia (Stecco et al, 2011, Stecco et al., 2014) [10,16,17]. HA is a high molecular weight polysaccharide in healthy tissues and is a key component of the ECM in the loose fascia, including between deep fascia and muscle, within muscles and between the collagen layers in the deep fascia. It is also a major component of articular joint synovial fluid, where it provides the viscoelasticity and lubrication to protect the joint cartilage. It is known that the concentration and composition of HA in the ECM of the fascia is associated with inflammation and joint problems (Temple-Wong et al., 2016) [14]. HA has an important significance for the slide and glide function and densification and adhesions in the fascia ECM are linked to reduced sliding ability (Langevin et al., 2011; Chaitow, 2014) [12,13]. Though HA has a non-Newtonian behavior, it is possible that the deep vibrations and pressure affect the viscosity of the HA to decrease, in a short time. Massage, manipulation, or physical therapies can cause disaggregation of the pathologic chain-chain interactions and a reversal of the aggregation of the HA fragments, by an increase of the subcutis temperature to 40° there is a change in viscosity (Stecco et al, 2013) [4]. Stecco et al. assume that this increase in temperature will not alter the quantity of HA but rather its structure and associative behavior. Treatment which only increases the temperature therefore gives short lasting effects. When HA is subjected to mechanical stress, such as manual deep friction or vibration, it is depolymerized, and lower molecular mass polymers are generated which help to restore the quality of HA and heal and re-establish a normal tissue sliding in the endo-, peri- and epimysium and deep fascia. This smaller HA polymers are highly inflammatory, angiogenic and immunogenic (Noble, 2002; Stecco et al, 2013, 2014) [4,16,17,26]. Stecco et al. suggest that manual manipulation with deep compression and friction is able to catalyze this reaction and that this self-resolving inflammatory reaction is the mechanism that restores the correct quantity and quality of substances in the fascia. The results indicate that myofascial treatment using a device generating deep pulsating vibrations reaches deeper in the tissue than manual manipulation and massage, but the physiological mechanism behind the successful treatments have to be further investigated. Ness et al. [27] and Usuki et al. [28] also have found that treatment with vibratory stimulation for spasticity gives promising results.
The study has a lot of deficits. It is a small study with a few patients, but it indicates a clear improvement in the ROM and the patients perceived reduced pain. Also, it is difficult to get patients to complete the treatment, as it may feel unjustified to continue as they have improved or got rid of their pain. There is also uncertainty with determining diagnosis, as there may be other underlying causes than FS to the shoulder problems. The duration period that the patients have had problems varies, which means that they have been in different phases (Hannafin et al, 2000) [1] and this most likely gives different effects of the treatment. Photographing and measurement of ROM are also a source of misinterpretation, in some cases the movement is not entirely pure abduction when the patients strain themselves and folded the body. Additional sources of error are the measurement of the angles with the protractor.
The study indicates that myofascial treatment with deep pulsating vibrations could be a valuable alternative for shortening the healing process and providing increased ROM and thus quality of life for patients diagnosed with FS. Using this type of treatment in the care process for these patients could be an easy and pleasant way to shorten the course of the disease. Further studies are recommended with larger patient groups as well as clinical studies to evaluate and validate the treatment effect in general and the findings of this study. If validated, a treatment method for patients with FS, could mean great socioeconomic benefits and an increased quality of life [29].
This study was initiated by physician Håkan B after discovering that more than fifty patients got increased mobility as a result of myofascial treatment with deep pulsating vibrations. As the main author, Håkan B receives no financial contribution and guarantees the publishing ethics and the unbiasedness of the study. Camilla RN has been working independently with myofascial treatment since 2015 and receives no financial contribution. Hans B has been working with myofascial treatment since 2012 and has invented the myofascial treatment devices and the treatment process used in this study.

![]()

 |
|
Patient ID |
Age |
Gender |
FS duration in months |
®ROM Day 1 before |
®ROM Day 1 after |
®ROM Day 7 before |
®ROM Day 1 after |
®ROM Day 37 before |
®ROM Day 1 after |
∆®ROM |
Full ROM |
Improved sleep |
FS01 |
52 |
W |
7-9 |
65 |
95 |
105 |
110 |
115 |
120 |
55 |
|
X |
FS02 |
57 |
W |
5-7 |
80 |
180 |
180 |
180 |
180 |
180 |
100 |
X |
|
FS03 |
42 |
W |
14-16 |
50 |
90 |
|
|
|
|
40 |
|
X |
FS04 |
41 |
W |
7-9 |
100 |
180 |
|
|
|
|
80 |
X |
|
FS05 |
51 |
W |
4-6 |
30 |
90 |
|
|
|
|
60 |
|
|
FS06 |
56 |
M |
6-8 |
80 |
120 |
125 |
140 |
140 |
150 |
70 |
|
X |
FS07 |
50 |
W |
6-8 |
65 |
130 |
75 |
115 |
|
|
50 |
|
X |
FS08 |
42 |
W |
5-7 |
65 |
90 |
95 |
110 |
95 |
110 |
45 |
|
X |
FS09 |
46 |
W |
5-7 |
135 |
180 |
180 |
180 |
180 |
180 |
45 |
X |
X |
FS10 |
48 |
W |
4-6 |
50 |
80 |
70 |
80 |
|
|
30 |
|
|
FS11 |
69 |
M |
10-11 |
75 |
90 |
80 |
90 |
80 |
100 |
25 |
|
X |
FS12 |
62 |
M |
1-2 |
100 |
180 |
115 |
170 |
140 |
140 |
40 |
|
|
FS13 |
89 |
W |
11-13 |
65 |
115 |
100 |
150 |
150 |
160 |
95 |
|
|
FS14 |
47 |
W |
9-11 |
70 |
140 |
150 |
160 |
180 |
180 |
110 |
X |
X |
FS15 |
49 |
W |
10-12 |
90 |
135 |
140 |
160 |
120 |
135 |
45 |
|
X |
FS16 |
47 |
M |
5-7 |
160 |
170 |
170 |
170 |
|
|
10 |
X |
|
FS17 |
47 |
W |
3-5 |
135 |
150 |
160 |
160 |
160 |
160 |
25 |
|
|
FS18 |
45 |
M |
22-24 |
100 |
170 |
140 |
180 |
180 |
180 |
80 |
X |
|
FS19 |
58 |
M |
12-14 |
135 |
160 |
130 |
170 |
130 |
170 |
35 |
X |
|
Patient ID |
Age |
Gender |
FS duration in months |
®ROM Day 1 before |
®ROM Day 1 after |
®ROM Day 7 before |
®ROM Day 1 after |
®ROM Day 37 before |
®ROM Day 1 after |
∆®ROM |
Full ROM |
Improved sleep |
FS20 |
68 |
W |
6-8 |
50 |
130 |
100 |
125 |
80 |
85 |
35 |
|
|
FS21 |
27 |
M |
3-5 |
70 |
160 |
135 |
180 |
180 |
180 |
110 |
X |
X |
FS22 |
42 |
W |
8-10 |
60 |
110 |
70 |
100 |
90 |
150 |
90 |
|
X |
FS23 |
45 |
M |
3-5 |
70 |
140 |
155 |
180 |
180 |
180 |
110 |
X |
X |
Table 1:Summary of the results
|
No |
>30° |
>45° |
>60° |
>90° |
Full |
Imp sleep |
Total |
23 |
20 |
16 |
12 |
9 |
9 |
14 |
Percent |
100 % |
87% |
70% |
52% |
39% |
39% |
61% |
Table 2: Increased ROM in degrees calculated on all 23 patients in the study
|
No |
>30° |
>45° |
>60° |
>90° |
Full |
Imp sleep |
Total |
17 |
15 |
13 |
12 |
10 |
9 |
12 |
Percent |
100% |
88% |
76% |
59% |
53% |
41% |
71% |
Table 3: Increased ROM in degrees calculated on 17 patients who continued the whole study




































