Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2019 Ghezzaz A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Pseudoxanthoma elasticum (PXE) is characterized by a progressive fragmentation and calcification of elastic fibers in connective tissue and when Bruch membrane (BM) is affected ocular modifications can be found. Recently, Optical coherence tomography-angiography (OCT-A) contribute to a better comprehension of lesions in PXE.
A 58-year-old woman presented with Pseudoxanthoma elasticum (PXE) complicated by choroidal neovascularization (CNV) in the right eye. Fundus examination found indirect signs of CNV associated with peau d’orange, angioid streaks (AS), Reticular pseudodrusen and subretinal fibrosis (SRF). Multimodal imaging confirmed the diagnosis of CNV and showed a hyper-reflective deposit on AS and SRF which expressed a vascular flow in OCT-A.
The subretinal deposits on AS and SRF are probably a fibrovascular tissue developed in response to the break of calcified Bruch membrane in PXE. OCT-A is a useful tool to distinguish CNV and allows a better comprehension of the reparation processes after a Bruch membrane break.
Keywords:Optical Coherence Tomography Angiography; Pseudoxanthoma Elasticum; Subretinal Fibrosis; Choroidal Neo vascularization; Angioid Streaks
List of abbreviations:AS: Angioid Streaks; BCVA: Best-Corrected Visual Acuity; BM: Bruch Membrane; CNV: Choroidal Neovascularization; FA: Fluorescein Angiography; ICGA: Indocyanine Green Angiography; OCT-A: Optical Coherence Tomography-Angiography; PO: Peau D’orange (PO); PXE: Pseudoxanthoma Elasticum; RPD: Reticular Pseudodrusen; RPE: Retinal Pigment Epithelium; SD-OCT: Spectral Domain- Optical Coherence Tomography; SRD: Serous Retinal Detachment; SRF: Subretinal Fibrosis
Pseudoxanthoma elasticum (PXE) is a rare systemic disease due to mutations in the ABCC6 gene that induces progressive fragmentation and calcification of elastic fibers in connective tissue and involve skin, the cardiovascular system and the eye. The first clinical sign is almost always small yellow papules on the nape and sides of the neck and in flexural areas. The cardiovascular system involvement result in intermittent claudication and peripheral artery disease, myocardial infarction or ischemic stroke [1]. On other hand, the ocular modifications are linked to the calcifications and the thickening of Bruch membrane (BM) which can take a form of peau d’orange (PO), retinal pigment epithelium (RPE) atrophy, angioid streaks (AS) and/or choroidal neovascularization (CNV) [2]. Furthermore, a Subretinal fibrosis (SRF) has also been reported in 7.8% of patients [3].
Recently, the apparition of the optical coherence tomography-angiography (OCT-A) contribute to facilitate the diagnosis additionally to a better comprehension of the physiopathology of lesions of PXE. Indeed, as it use a decorrelation signal, OCT-A detect blood cells movement and permit a good visualization of the CNV without invasive injections as well as it can explore the choriocapillaris which is tightly attached to BM [4]. Corbelli et al. reported the presence of a hyper-reflective subretinal deposit with a flow signal in OCT-A in some cases of AS [5] . However, the nature of this deposit still not well known. In this work, we report the utility of a multimodal imaging including OCT-A in the diagnosis and the physiopathology comprehension of ocular PXE complicated by AS, SRF and CNV.
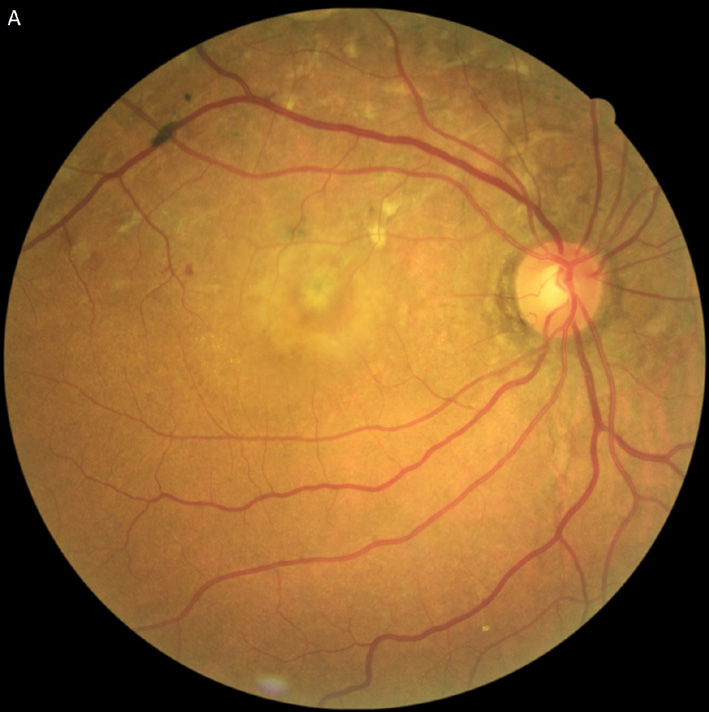
A 58-year-old woman native from Haiti and presenting foveal CNV developed in the right eye was referred to our institution. The best-corrected visual acuity (BCVA) was at 20/100 in the right and 20/20 in the left eye. Intraocular pressure was 15 mm Hg and slit lamp biomicroscopy was normal in both eyes. Upon fundus examination, PO was noted, along with a circular and linear AS around the optic disc in both eyes. However, they were more peripheral in right eye and were associated to a serous retinal detachment (SRD) and macular edema. A large chorioretinal yellowish patch with an irregular and spiked shape that correspond to the so-called SRF was noted in the superior field of the right eye, while it was located in the nasal field in the left eye (Figure 1) in association with reticular pseudodrusen (RPD).
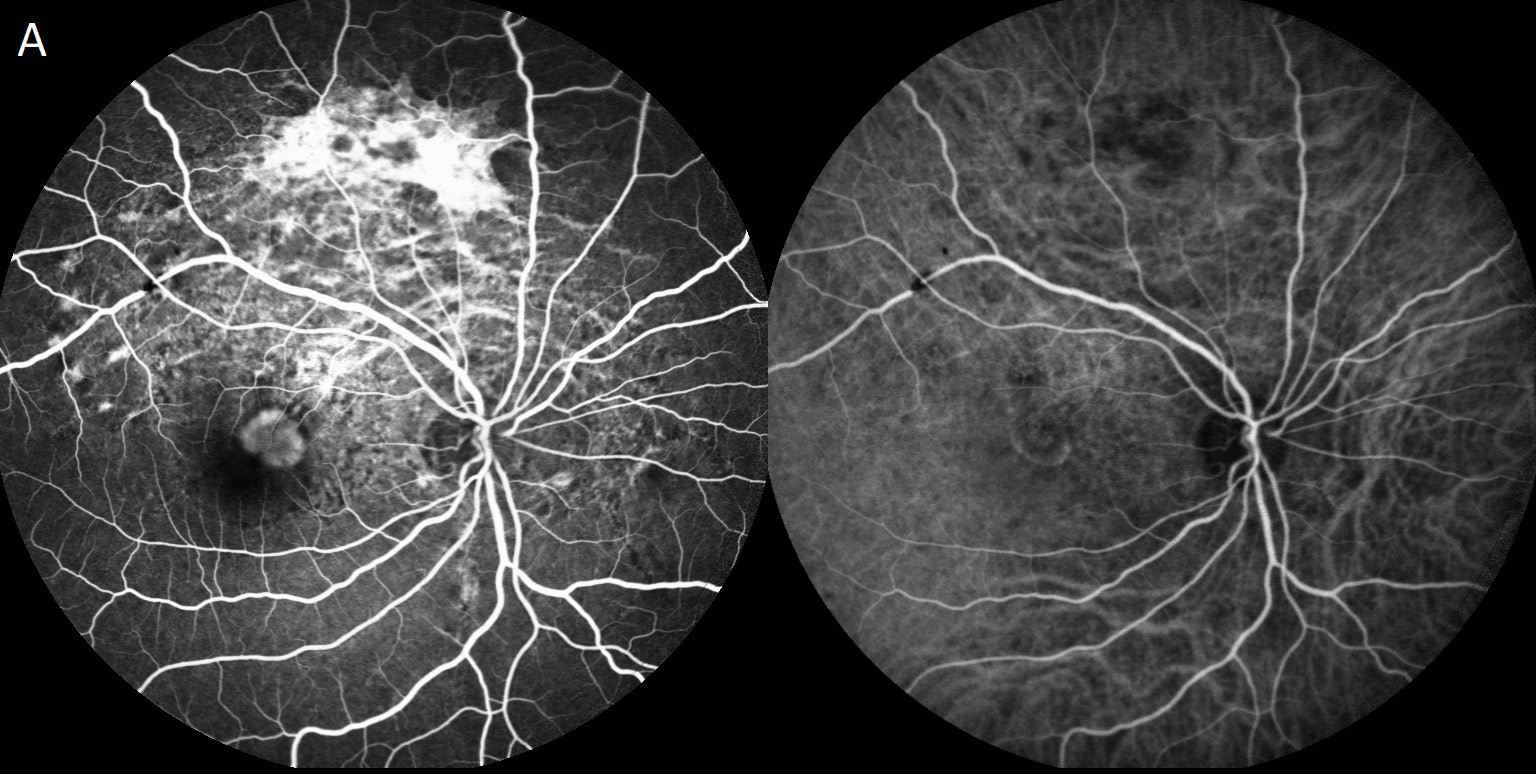
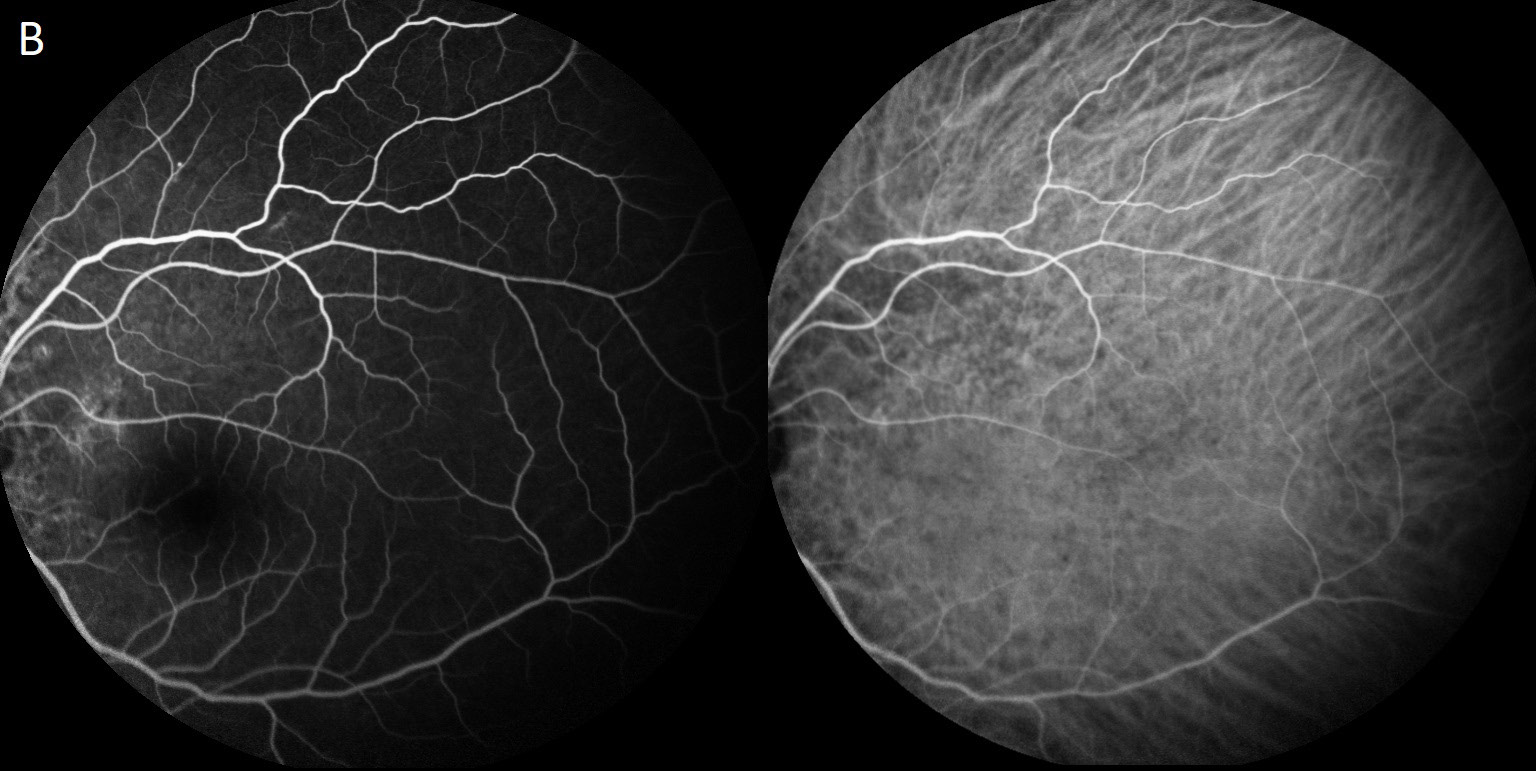
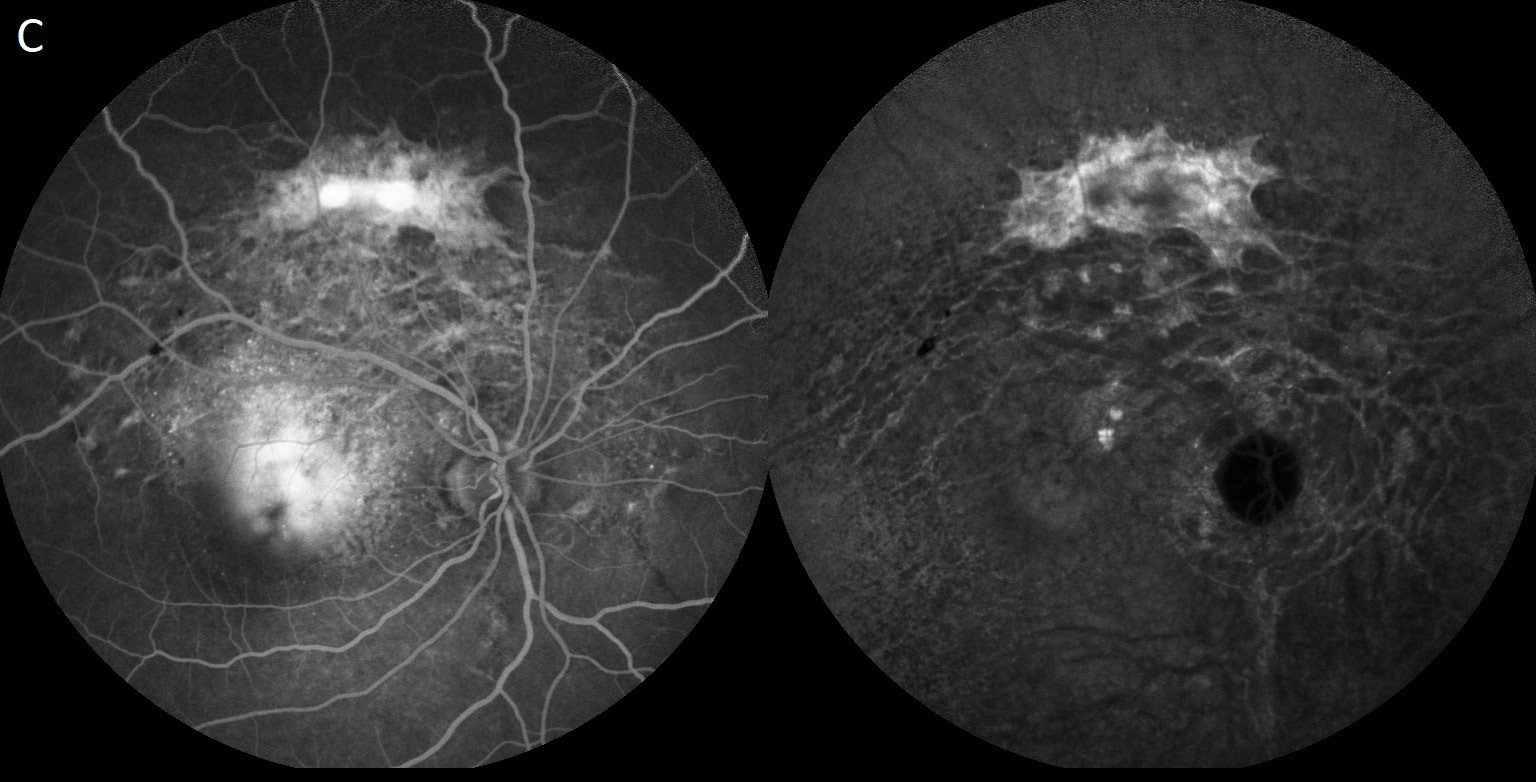
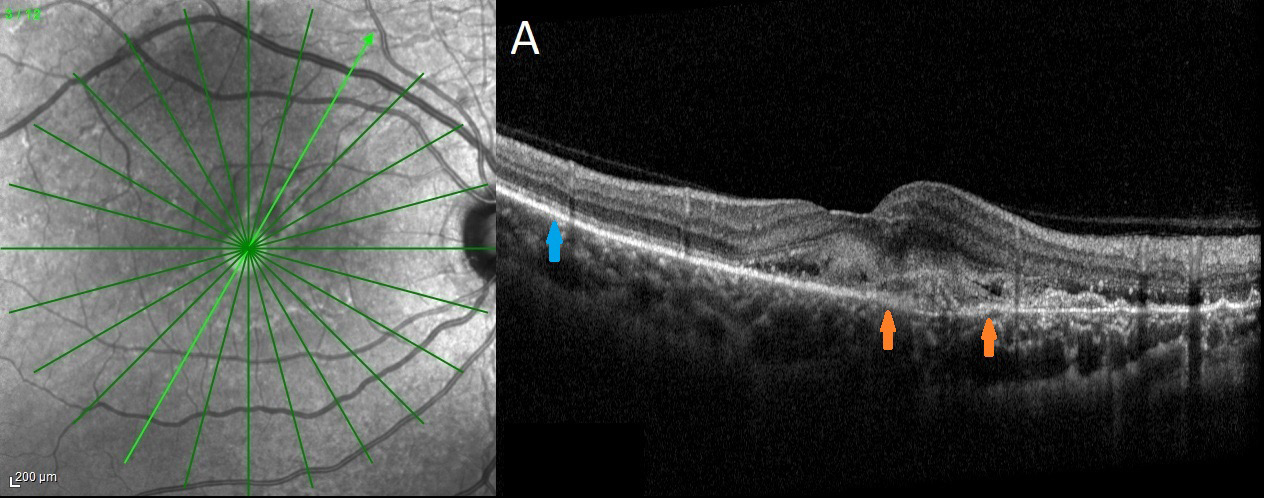
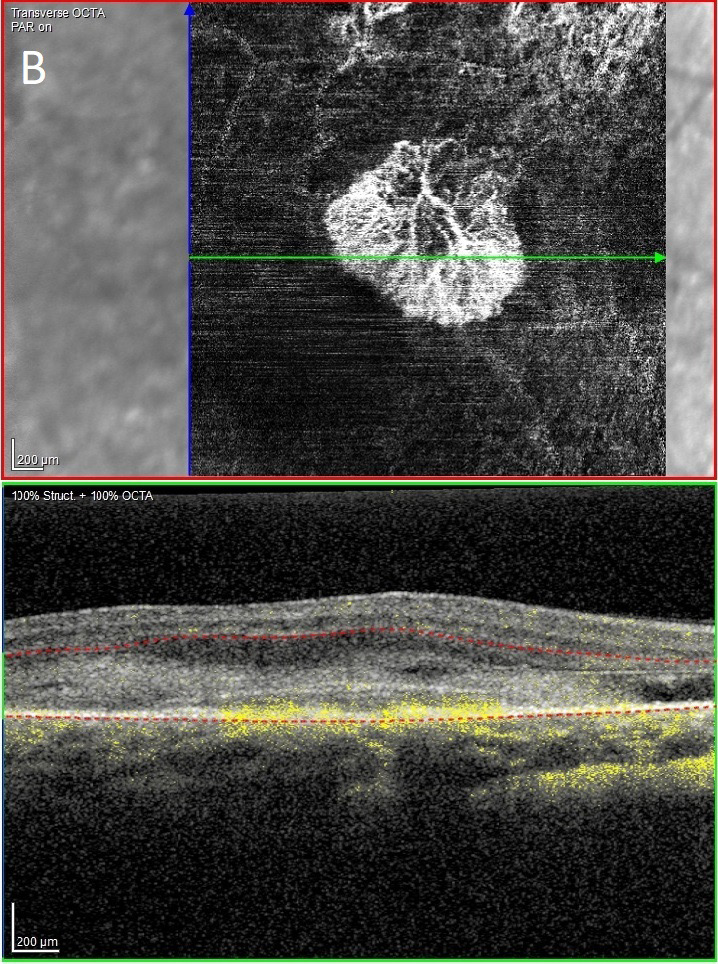
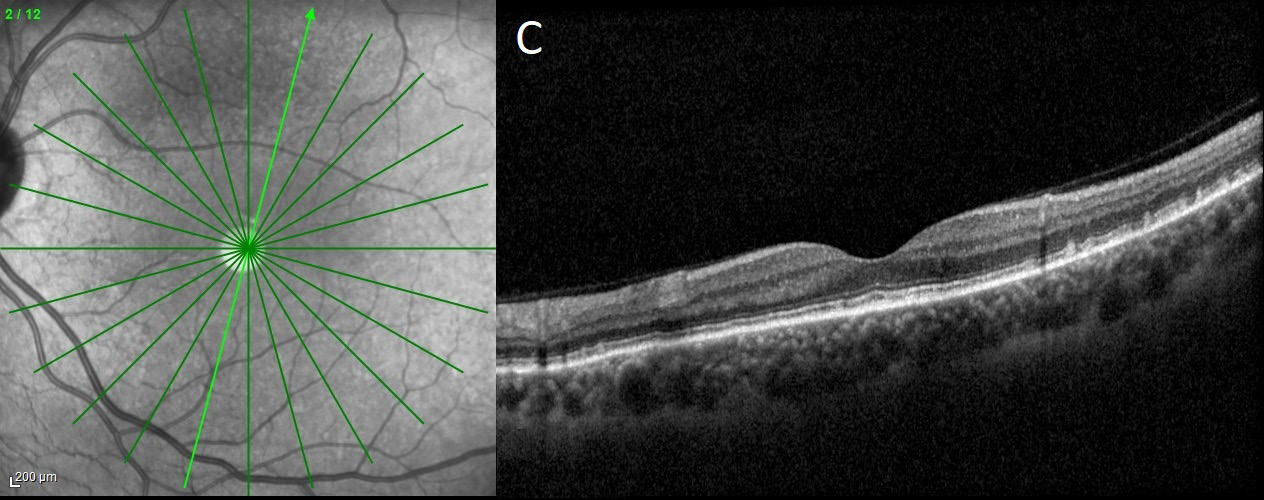
In indocyanine green angiography (ICGA), SRF and AS were hypofluorescent in early periods and become hyper-fluorescent in later times, while a hyperfluorescence aspect was noted during all the sequence of fluorescein angiography (FA) (Spectralis, HRA + OCT, Heidelberg, Germany). This aspect contrasted with the hypofluorescence observed in the posterior pole and around the papilla in both eyes. The latter was more important in the right eye and included the macula (Figure 2). Indirect signs of CNV were visible in the spectral domain- optical coherence tomography (SD-OCT) (Spectralis, HRA + OCT, Heidelberg, Germany) in the form of an hyper-reflective deposit in the fovea above RPE which was surrounded by SRD and macular edema. This macular CNV were detected in FA and ICGA and were also clearly visible in OCT-angiography, taking a sea-fan shape, emerging from a retro-epithelial feeding vessel in association with AS. Interestingly, Scans of the SD-OCT passing over SRF and AS showed an hyper-reflective subretinal deposits under outer retinal layers, which appears in OCT-A as a homogenous vascular network in connection with AS (Figure 3).
Skin examination found typical lesions in the neck and the diagnosis of PXE was confirmed by the identification of an ABCC6 gene mutation. A five monthly intravitreal injections of aflibercept (40 mg/mL) were performed in the right eye. At the last assessment 9 months later, BCVA worsened to 20/200 in the right eye in consequence of the atrophy and the tubulations in the outer retina despite the absence of CNV activity.
Central vision in PXE patients can be threatened by the presence of CNV or atrophy of the outer retina and RPE. Generally, a specific fundus features such as PO, AS, SRF or pattern dystrophy are found separately or in association depending to the stages of the disease [3]. PO are present in early stages in the posterior pole probably due to the unevenness calcifications and thickening of BM before becoming more uniform and extends to the periphery. This is clearly visible in the late phases of ICG-angiography in the form of three concentric zones, with a central hypofluorescent zone due to disruption of ICG capitation by RPE and BM, followed by a speckled zone corresponding to PO and a normal fluorescent zone [6]. Subsequently, BM becomes more vulnerable to small stretches that can lead it to break. This results in AS, which predominates around the papilla and posterior pole, without overstepping the transition zone of PO. However, the break can be more important, leading to a phenomenon called SRF, which is clearly visible in the present case in both eyes as a yellow patch in the transition zone connected to the AS network.
Prior studies described SRF as a rare feature in PXE and are presumed due to a large break in BM in association with fundus pulverulentus [3,7]. In this case, SD-OCT found SRF as an hyper-reflective deposit under the outer retina. This aspect was also observed in AS which also shares the same presentation in FA and ICGA. Interestingly, a decorrelation signal and intrinsic flow was found in this patch in OCT-angiography in SRF that most probably corresponds to a vascular network. This observation was also found in peripapillary and centrifugal AS. The absence of SRD or retinal edema surrounding the SRF and AS were not an argument in the favor of a peripheral CNV.
As a decorrelation flow is believed due to blood circulation [8], the probable hypothesis of this observation is that SRF corresponds to a fibrovascular tissue developed in reaction to a large break in BM. The observation of the same aspect in some cases of AS in previous studies is concordant with this hypothesis [5]. However, the other hypothesis is that SRF are the consequence of a local protrusion of choriocapillaris through a large defect of the BM in the form of a patch, while linear defects of BM in AS are too small in most cases to allow the protrusion. However, the hypofluorescent aspect in the early phases of ICGA more likely indicate a mask effect of fibrovascular tissue rather than normal choriocapillaris. This fibrovascular tissue is impregnate by indocyanine which give a hyperfluorescent aspect in the late phases.
AS increases the risk of type 2 CNV in the consequence of BM break in the macula [9]. In our observation, CNV were clearly visible in OCA-A as a vascular network, taking a sea-fan shape connected to AS. After three intravitreal injections of aflibercept, BCVA was worsened, despite the resorption of SRD and CNV in OCT-A, explained by the presence of tabulations in outer retinal and a macular atrophy which are well known as factors of a limited VA recovery [10]. Finally, the better detection of RPD in the left eye can be explained by the presence of scars in the right eye which reduce their detectability. However, the location of these RPD in the central hypofluorescent zone is probably due to the impairment of BM in the macular field where the chorio-retinal exchange are more important [11,12]. However, the predictability of their presence for the development of CNV is not well known.
Prior reports showed the contribution of OCT-A in cases of CNV in PXE, even in the absence of exudation [13,14]. However, to the best of our knowledge, only a few reports have shown interest in the contribution of OCT-A for other fundus features in PXE and specifically SRF. The breaks of the fragile BM can be accompanied by tissue changes to limits the consequence of an important BM defect. Further studies using a multimodal imagery and OCT-A are needed to confirm this observation.
Ghezzaz A and Mahdjoubi A: Conception, design, acquisition of data, analysis and interpretation of data; Sigal M-L: Acquisition of data, analysis and interpretation of data; Brodard F: Acquisition of data, analysis and interpretation of data; Idlefqih W: Acquisition of data, analysis and interpretation of data; Chahed S: Conception, design, acquisition of data, analysis and interpretation of data.

![]()

 |
 |
|
|
|
 |
 |
|
|
 |
Figure 1: Fundus aspects: (A and B): Peau d�orange aspects in both eyes associated with serous retinal detachment and macular edema in the right eye and reticular pseudodrusen in the left eye; (C, D and E): Angioid streaks were around the papilla and spread in the centrifugal network. Subretinal fibrosis in the superior field of the right eye and the nasal field in the left eye as a yellow specked patch in connection with angioid streaks |
|
 |
|
|
 |
|
|
 |
|
|
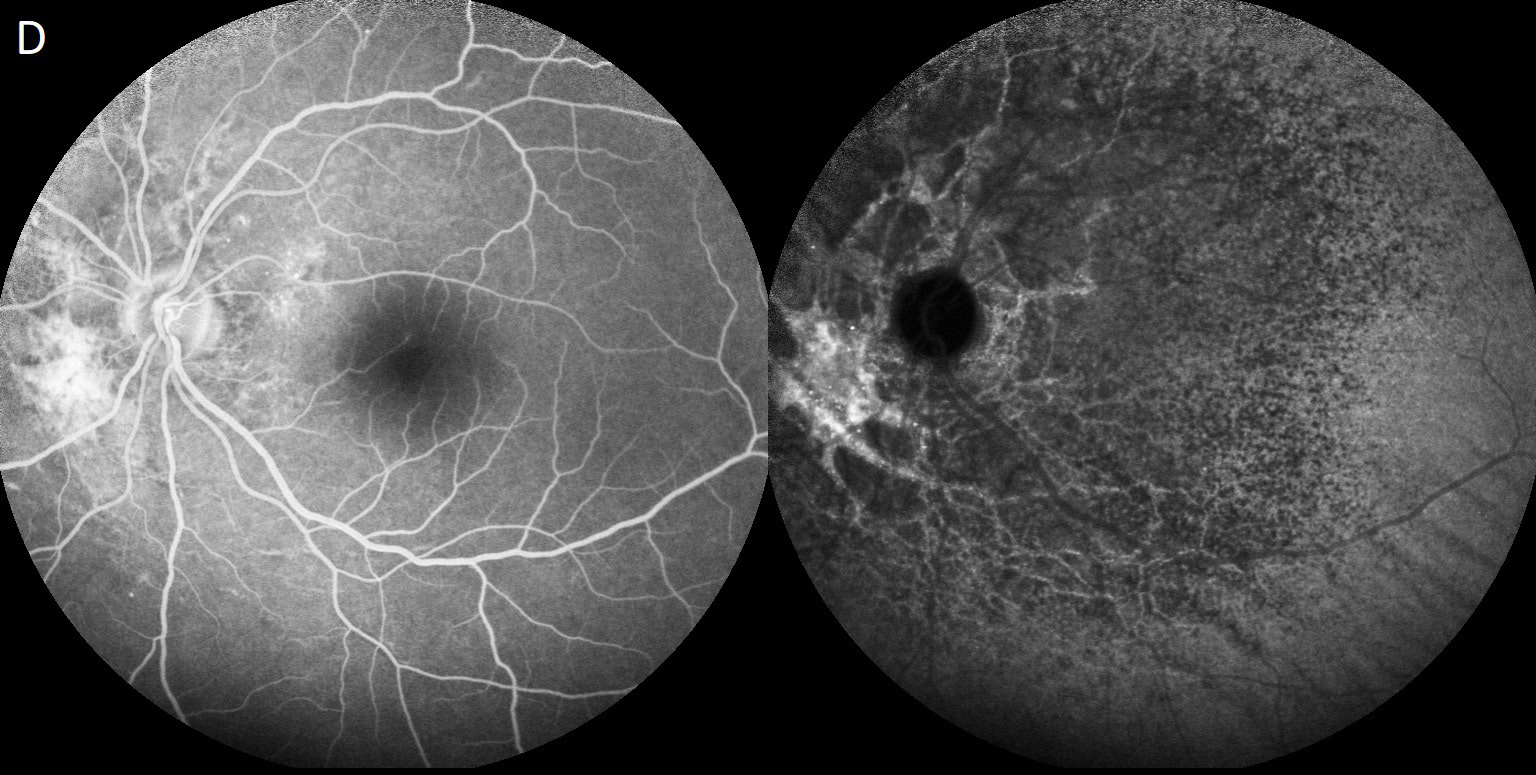 |
Figure 2: Indocyanine green angiography (ICGA) and fluorescein angiography (FA): (A and B): Early phase: Choroidal neovascularization was clearly visible in ICGA and FA in the right eye. Subretinal fibrosis showed hypofluorescent aspects in ICGA while it was hyperfluorescent in FA as angioid streaks; (C and D) Late phase: A hypofluorescent aspect in the posterior pole was noted in both eyes but was more important in the right eye and contrasted with hyperfluorescence of angioid streaks and subretinal fibrosis |
|
 |
|
|
 |
|
|
 |
|
|
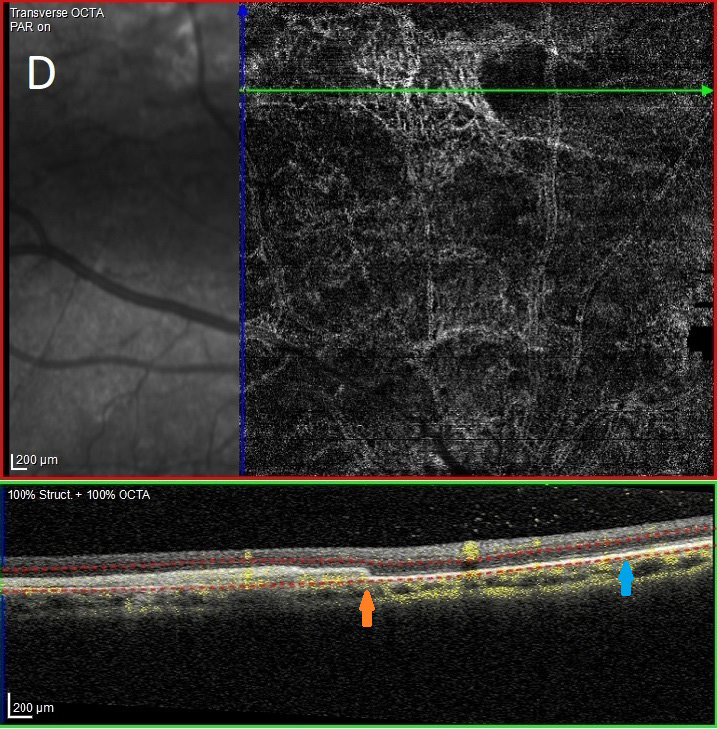 |
Figure 3: OCT-Spectral domain and OCT-angiography: (A, B and C): Indirect signs of the CNV were visible in the OCT-spectral domain in the right eye while the CNV were clearly visible in OCT-A taking the shape of a sea-fan in connection with the retro-epithelial part which is associated with the angioid streaks. In the B-Scan, the yellow spots represent the projection of the vascular flow detected in OCT-A. The blue arrow shows the unbroken BM while the orange arrow indicates its interruption. In the left eye, no macular anomaly was noted except for the presence of pseudoreticular drusens in the supero-temporal field; (D and E): Subretinal fibrosis appears as an hyper-reflective subretinal deposits between the outer retinal region and BM that appears in OCT-A as a homogenous vascular network in connection with AS. Here also, the blue arrow shows the unbroken BM while the orange arrow shows its interruption |




































