Open Access
Case Report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2017 Sandeep Reddy J. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Corrosive injuries of the Upper gastrointestinal tract (UGIT) are common in developing countries mostly mortality and morbidity is high in India due to suicidal attempts. In this case series, a 17 years old female and 51 year old male subject intentionally self-harmed by ingesting toilet cleaner containing higher amounts of hydrochloric acid and presented to the emergency department of tertiary care hospital and the different aspects of the case are discussed in detail in this paper.
Keywords: Upper Gastrointestinal Tract; Mortality; Morbidity; Toilet Cleaner
Corrosive injuries of the Upper gastrointestinal tract (UGIT) are common in developing countries, mostly mortality and morbidity is high in India due to suicidal attempts. Both acid and alkali substances when consumed, it causes significant injury to the upper gastrointestinal tract. The extent of injury depends upon several factors such as nature of the offending agent, amount, concentration and duration of exposure [1].
Acid ingestion: Causes coagulation necrosis. In this process, hydrogen (H+) ions desiccate epithelial cells producing an eschar. This process leads to edema, erythema, mucosal sloughing, ulceration and necrosis of tissues [2].
The conventional acceptance that acids preferentially damage the stomach, due to the protective esophageal eschar, has recently been questioned, with observation of extensive esophageal damage and perforations after acid ingestion [3]. Likewise, compared with alkali, ingestion of a strong acid may be associated with a higher incidence of systemic complications, such as renal failure, liver dysfunction, disseminated intravascular coagulation and hemolysis [4].
Esophageal injury begins within minutes and may persist for hours. Initially, tissue injury is marked by eosinophilic necrosis with swelling and hemorrhagic congestion [5].
A 17-year-old female intentionally self-harmed by ingesting toilet cleaner containing higher amounts of hydrochloric acid and presented to the emergency department of tertiary care hospital with the complaints of hematemesis, throat pain, nausea, burning sensation. Endoscopy was done and report shows Corrosive injury of oropharynx & UGIT severe injury of GE junction & Stomach (Figure 1).
Treated with injection pantoprazole 40mg OD, syrup sucralfate 10ml on day-1. On day-2 C/o epigastric tenderness, nothing by mouth, pantoprazole infusion was started 80mg @ 4.0 ml/hour. On day-3 C/o mild throat pain, dysphagia. On day-4 to day-6 observation and discharged with suitable medications.
A 51-year-oldmale intentionally self-harmed by ingesting 10ml toilet cleaner containing 5 ml of hydrochloric acid and presented to the emergency department of tertiary care hospital with the complaints of hematemesis, dysphagia, throat pain, nausea, chest discomfort. Endoscopy was done and report shows Corrosive injury of larynx & UGIT severe injury of esophagus& Stomach (Figure 2).
Treated with injection pantoprazole 40mg OD, syrup sucralfate 10ml, injection thiamine 1g in 100ml normal saline, injection cefotaxime 1g and nothing by mouth on day-1. On day-2 C/o hematemesis. On day-3 C/o hematemesis mild throat pain, dysphagia. On day-4 C/o hematemesis decreased but dysphagia. On day-5 c/o dysphagia, aversion therapy, injection lorazepam 1cc SOS was started to stop alcohol consumption and behavior. On day-6 to 7 observation and discharged with suitable medications.
In some cases, several symptoms such as laryngeal edema, pulmonary edema, shock, gastrointestinal perforation, acidosis, electrolyte abnormality, or disseminated intravascular coagulation (DIC) may occur. However, specific therapies for acid ingestion do not exist, and general management by controlling breathing and circulation and treatment based on the symptoms is provided for patients [6]. The mortality rate is between 10% to 20% and rises to 78% in cases of attempted suicide [7]. Ingestion of corrosive substances either accidentally or intentionally for the purpose of suicide is a common form of poisoning in India because of easy access to acids as they are used as cheap toilet cleansers [8,9].
Esophagogastroduodenoscopy is considered crucial and usually recommended in the first 12-48 h after caustic ingestion, though it is safe and reliable up to 96 h after the injury [4,10]; gentle insufflations and great caution are mandatory during the procedure. Endoscopy and even dilatation have been performed without consequences from 5 to 15 d after corrosive ingestion [11]. To date, the efficacy of proton-pump inhibitors and H2 blockers in minimizing esophageal injury by suppressing acid reflux has not been proven, though an impressive endoscopic healing after IV omeprazole infusion has been observed in a small prospective study [12].
The administration of broad-spectrum antibiotics is usually advised mainly if corticosteroids are initiated, as well as if lung involvement is identified [13,14]. In this case series we report two patients with different age and gender variants who are intentionally self-harmed by ingesting toilet cleaner (10ml) containing higher amounts of hydrochloric acid (5ml) due to their low socioeconomic status, diagnosed endoscopically and treated with suitable therapy.

![]()

 |
Figure 1: (A) Esophagus - Erosions & superficial ulceration with exudates; (B) Stomach - Erosions with oozing of blood; (C) Large ulcer with black base extending into antrum |
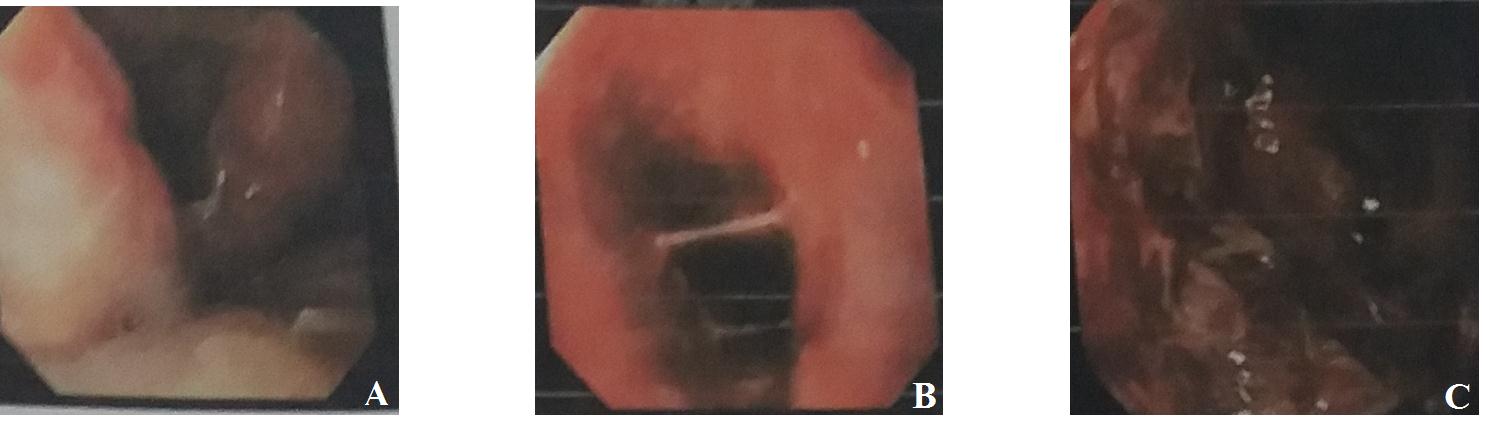 |
Figure 2: (A) Esophagus - Diffuse circumferential superficial ulcers & Hemorrhages; (B and C) Stomach and Duodenum - Hemorrhages with superficial ulcers and black exudates |




































