Open Access
Case Report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2016 Kataria SP. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
A 13 year old, premenarchal, previously healthy girl presented to the emergency department of our hospital with complaints of vomiting, constipation and abdominal pain for past one day. The patient also complained of slowly increasing abdominal distension and mild abdominal discomfort since past four months. Patient was taken up for laparotomy. A cystic solid pelvic mass was present originating from right ovary. Unilateral salpingoophorectomy with tumor removal was performed. The tumor measured 25x20x15 cm and weighed 3.5 kilograms. Specimen was sent for histopathological examination and diagnosis of mucinous cystadenoma was made.
Keywords: Giant mucinous cystadenoma adolescent
Abbreviations: CM: Centimeter
Mucinous cystadenomas account for approximately 10-20% of all epithelial ovarian tumours. About 75-80% of these tumours are benign [1]. They are usually seen between the third and fifth decades and 5-10% of them are bilateral. These benign tumours are rare entity in adolescents. The majority of ovarian masses in adolescent patients are non-epithelial in origin, with a predominance of germ cell tumours, while epithelial neoplasms make up a small proportion of ovarian masses in this age group [2,3]. Here we report a giant ovarian mucinous cystadenoma in an adolescent, the seventh largest mucinous cystadenomas reported in the literature.
A 13 year old, premenarchal, previously healthy girl presented to the emergency department of our hospital with complaints of vomiting, constipation and abdominal pain for past one day. The patient also complained of slowly increasing abdominal distension and mild abdominal discomfort since past four months. On physical examination, a huge, well defined, immobile pelvic mass was palpable which filled the whole pelvis and abdomen and extended upto xiphoid process. The sonographic appearance of the tumor was predominantly multicystic with some solid regions at the margin. There was minimal intra-abdominal fluid located around the tumor. Uterus was depressed and displaced by the tumor. Left ovary appeared normal. Routine hematological and biochemistry tests were within normal limits. Patient was taken up for laparotomy. A cystic solid pelvic mass was present originating from right ovary. Examination of the pelvis, abdominal walls, diaphragmatic surface and peritoneum did not show presence of implants and metastasis. Unilateral salpingoophorectomy with tumor removal was performed. The tumor measured 25x20x15 cm and weighed 3.5 kilograms (Figure 1). Specimen was sent for histopathological examination; where cyst wall revealed the presence of columnar epithelium overlying ovarian stroma. The epithelium was tall columnar, with basal nuclei and abundant intracellular basophilic mucin. A final diagnosis of mucinous cystadenoma was made. Postoperative recovery was uneventful and the patient was discharged on the sixth postoperative day. Menarche occurred six months later. The patient is being followed up regularly and there has been no evidence of recurrence after 36 months of surgery.
Ovarian neoplasms may be divided according to original cell types into three main groups: epithelial, sex cord stromal cell, and germ cell. Taken as a group, the epithelial tumors are by far the most common type. The most common types of epithelial neoplasms are benign cystadenoma of which 75% are serous cystadenomas and 25% are mucinous cystadenomas. Serous or mucinous cystadenomas of the ovary, benign or malignant, are rare in children. They arise from mullerian germinal epithelium. Patients are usually post-pubertal [1,4].
Mucinous cystadenoma of the ovary; a benign neoplasm accounts for 15% of all ovarian neoplasms. Being most prevalent in third to fifth decade, its incidence in adolescents is a rarity. These neoplasms vary in size from few centimeters to several centimeters and can weigh as heavy as a few kilograms. Grossly, mucinous neoplasms are characterised by cysts of variable sizes without surface invasion. Histologically, mucinous cystadenoma is lined by tall columnar non-ciliated epithelial cells with apical mucin and basal nuclei. They are classified according to the mucin-producing epithelial cells into three types. Mucinous neoplasms are classified into three types according to mucin producing epithelial cells namely endocervical, intestinal and mullerian [5]. Mucinous tumours are usually cystic, with 76% being multilocular and 24% unilocular. Only approximately 10% of mucinous tumours are bilateral, excluding metastatic spread to the contralateral ovary [5,6].
Differential diagnosis of ovarian masses in adolescence includes cyst formation, ovarian torsion, benign or malignant ovarian neoplasm and involvement of the ovary in lymphoma, leukaemia or metastatic disease [2] (Figure 2). Malignant transformation of these tumors is a rare event and has been reported in 5-10% of cases. Because of this potential, these tumours must be histologically classified and appropriately treated [1,3].
Management of ovarian cysts depends on the patient’s age, the size and structure of the cyst and menopausal status. Conservative surgery is the treatment of choice in younger patients due to the low rate of malignant transformation. Though cystectomy has a greater chance of preserving fertility, is associated with higher recurrence rate. Salpingo-oopho- rectomy has thus been recommended as fertility-sparing surgery. Patient should be followed up carefully for recurrence, especially if tumor was not completely removed by surgery. Prognosis though excellent for these tumors, careful follow up is mandatory due to risk of recurrence [7,8].
In our patient, the mass was enormous in size and there was no normal ovarian tissue grossly. Therefore, right salpingo- -oophorectomy was performed. The patient is being followed up regularly and there has been no evidence of recurrence after 36 months of surgery.

![]()

 |
| Figure 1: Giant Mucinous Cystadenoma Weighing 3.5 Kilograms |
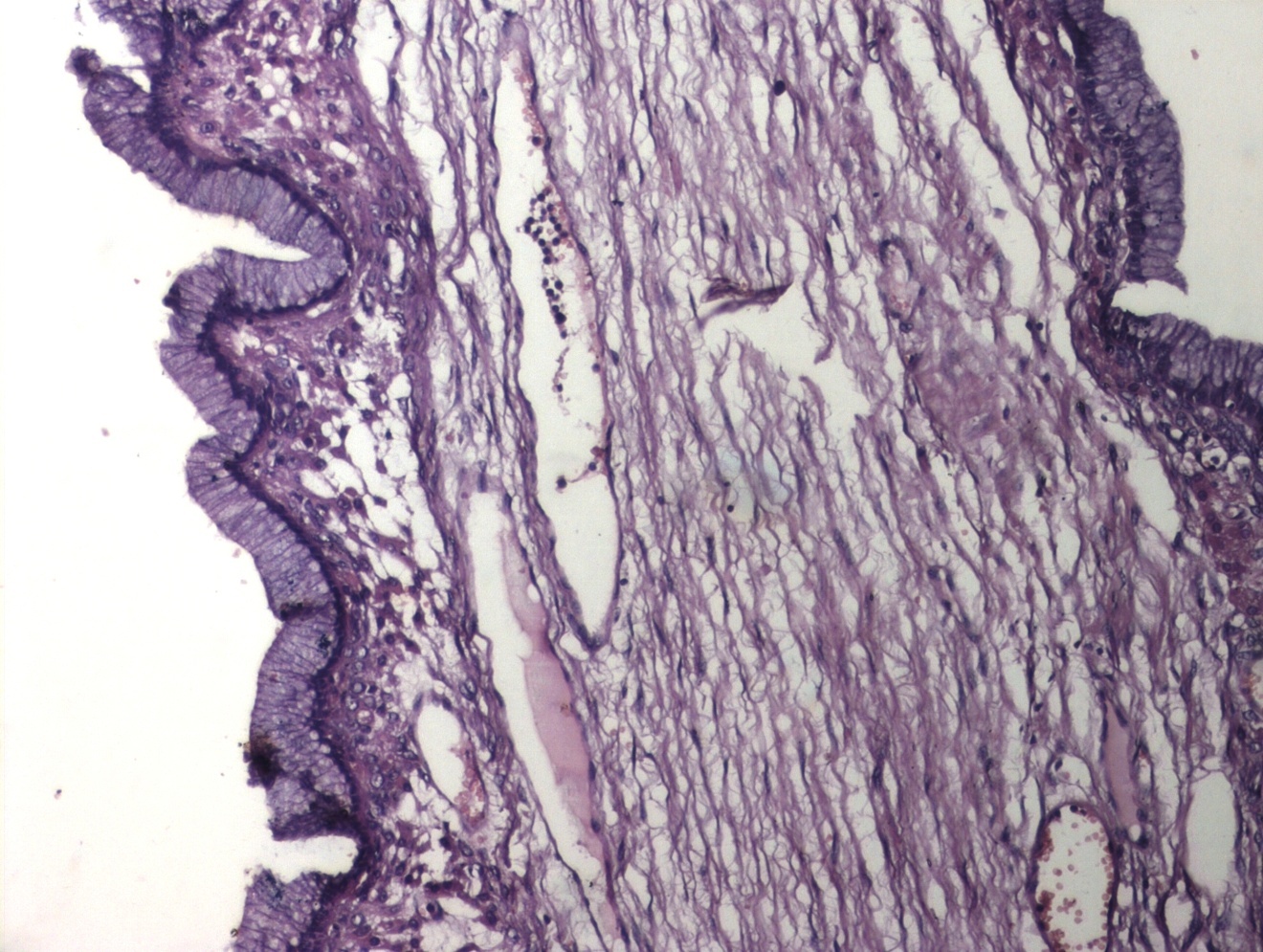 |
| Figure 2: Mucinous Cystadenoma Ovary (H&E, 100x) |




































