Open Access
Research Article
Max Screen >>
ISSN: 2576-7623
Copyright: © 2016 Tas B. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
To compare three different types of volumetric modulated arc therapy (VMAT) planning tecniques using Elekta Versa HD lineer accelerator to deliver total body irradition (TBI) treatment on the coach and to evaluate feasibility of VMAT planning tecnique for TBI treatment.
Five TBI patient’s treatment planning performed using Monaco5.1® treatment planning system with three different VMAT tecniques for each patient. First one was single arc VMAT tecnique, second one was dual arc VMAT tecnique and third one was 2 fields arc VMAT tecnique for one isocentre. The VMAT-TBI tecnique consisted of three isocentres and three overlapping arcs. Eight TBI patient’s treatment planning system (TPS) was performed with the best VMAT technique which we determined. The prescribed dose was 12 Gy. Mean dose to lungs and kidneys were restricted less than 10 Gy and maximum dose to lens were restricted less than 6 Gy. X-ray volume imaging (XVI) cone beam computer tomography (CT) was used as an image guided radiation therapy (IGRT) method for each VMAT delivery, in addition, C-RAD surface guided radiotherapy (SGRT) device was used for patient positioning and monitoring. The plans were verified using 2 Dimensional array and ion chamber for patient quality assurance (QA). The comparison between calculation and measurement were made by γ-index analysis and absolute dose.
This study demonstrates that dual arc VMAT technique has got less monitor units (MUs) than other techniques but an average delivery time is %17 more than single arc VMAT technique. When we compared organ at risk (OAR)s, we had less dose and better dose coverage to target with dual arc VMAT technique. An average total delivery time was determined 923 ± 34 seconds and an average MU was determined 2614 ± 228 MUs for eight TBI patient’s dual arc VMAT. Mean dose to lungs was 9.7 ± 0.2 Gy, mean dose to kidneys was 8.8 ± 0.3 Gy, maximum dose to lens was 5.5 ± 0.3 Gy and maximum point dose to patient was 14.6 ± 0.3 Gy, hetereogenity index (HI) of planning target volume (PTV) was 1.13 ± 0.2, mean dose to PTV was 12.6 ± 1.5 Gy and mean γ-index pass rate was %97.1 ± 1.9.
The results show that the tecnique for TBI using VMAT on the treatment coach is feasible with dual arc VMAT tecnique on the coach.
Keywords: TBI, VMAT
Total body irradiation (TBI) is designed to irradiate the whole body uniformly to a prescribed dose while minimizing radiation induced complications to lungs and other normal organs. TBI with megavoltage photon beams is one component used in treating several diseases, including multiple myeloma, leukemias, lymphomas and some solid tumors [1,2]. Also, conjuction with chemotherapy is widely used as a conditioning regimen before bone marrow transplant (BMT) for patients with hematologic malinancies. In combination with chemotherapy demonstrates superior treatment outcomes for BMT conditioning compared with chemotherapy alone [3-7]. TBI provides a uniform dose of radiation to the entire body, penetrating areas such as the central nervous system (CNS) and testes, where traditional chemotherapy is ineffective [8]. The purpose of this treatment is threefold: to eliminate residual cancer cells, to provide space for stem cell engraftment through bone marrow depletion, and to prevent rejection of donor stem cells through immunosuppression [9,10].
Studies in mice and humans show that the toxicities of TBI can be improved further by fractionating the radiation. The rate of lung repair between fractions was reviewed by Travis [11], indicating the presence of two significantly different repair rates corresponding to a fast repair half time of 0.40 hours and a slow half time of 4.01 hours. The slow repair component needs to be kept in mind when designing TBI schedules that include two or three fractions per a day [12]. The ideal dosing schedule depends on patient age, disease and the intended type of stem cell transplant [7]. Recommended dose schedule for myeloablative TBI is 12 to 15 Gy given in 8 to 12 fractions over 4 days, with 2 to 3 treatments daily doses > 15 Gy have been shown to decrease relapse rate, but also increase the incidence of graft vs. host disease and decrease 2 years survival [8]. Low-dose TBI, with doses of 2 to 8 Gy given in 1 to 4 fractions in combination with chemotherapy, is an effective conditioning regimen for hematopoietic stem cell transplantation in patients who cannot tolerate myeloablation due to age or comorbidities [8,13,14]. A randomized study from Seattle in the setting of AML compared single dose TBI (10 Gy) to a fractionated schedule (2 Gy for six fractions). The last update of this trial showed significant superiority of the fractioanated scheme in terms of every free survival [15]. Another Seattle randomized trial of AML in first remission compared fractionated TBI doses of 12 Gy with 15.75 Gy, showing a decreased relapse rate from 35% to 12%, but at the expense of a significant increase in therapy related mortalit, resulting in no survival advantages to a higher radiation dose [16].
Many different tecniques have been described for effective irradiation of the whole body and indeed improvements in both the irradation tecnique and physical dosimetry. Most of the current TBI procedures are based on tecniques established on linear accelerators that are used for conventional radiotherapy. The large photon fields are generally achieved by treating the patient at extended SSD with standart linear accelerators or with special dedicated machines. The variable SSD available at current radiotherapy facilities is partially responsible for the variation in TBI tecniques and procedures. Equipment Guidelines recommend the use of parallel opposed pairs of high-energy photon beams from 4 to 18 MV for TBI [2]. TBI tecniques typically comprise a combination of various opposing field setups in a sitting or lying patient position at very extended SSDs. The extended SSD tecnique using a single large field encompassing the entire patient is by far the simplest and the most prevalent TBI tecnique used today. It eliminates the dosimetry complications in regions of field junctions introduced by using multiple small fields and concern that cells circulating through the body could potentially receive a reduced dose. These tecniques use Standard radiotherapy linear accelerators (LINAC)s and rely on a maximum collimator setting, a large SSD, and beam divergence to produce the large irradiation field required for TBI. AAPM’s TG-51 calibration protocol provides guidelines for dosimetry of high-energy photon beams [17]. Recent studies demonstrate the efficacy of helical tomotherapy for decreasing TBI treatment time and increasing homogeneity of delivered radiation [18]. Helical tomotherapy (HT) allows for irradiation of large target volume at nominal source axis distance (SAD), without additional requirements on treatment room size or shielding. HT consists of a linac mounted on a computed tomography (CT) gantry and delivers a fan beam (up to 5 cm x 40 cm) modulated with binary 64-leaf multileaf collimator (MLC). The beam source continuously rotates in the gantry while the couch is translated through the bore, which generates a helical pattern that can cover a treatment length of up to 160 cm. Because of their limited body length the tecnique seems especially eligible in juvenile patients.
In our study, we investigated the use of Linac-Based TBI by VMAT at nominal SAD technique on the coach. Five TBI patient’s treatment planning performed using Monaco5.1® treatment planning system with three different VMAT tecniques for each patient. First one was single arc VMAT tecnique, second one was dual arc VMAT tecnique and third one was 2 fields arc VMAT tecnique for one isocentre. The VMAT-TBI tecnique consisted of three isocentres and three overlapping arcs. Eight TBI patient’s TPS were performed with the best VMAT technique which we determined.
For treating patients, Versa HD® (Crawley, Elekta) linear accelerator with 6 MV, equipped with Agility® collimator system, XVI 5.0 cone beam CT was used as an image guided radiation therapy (IGRT) method for each VMAT delivery, also, Sentinel® (Sweeden, C-RAD) laser based surface guided radiotherapy (SGRT) device was used for patient positioning and monitoring. This is shown Figure 1.
Agility® collimator system included 160 MLC, minimum leaf width was 5 mm, maximum field size was 40 x 40 cm2 at nominal SAD:100 cm. MLC’s effective speed was 6.5 cm/second and leaf travel was 15 cm over the central axis. VMAT plans were generated on Monaco 5.1® (Crawley, Elekta) treatment planning system with Monte Carlo algorithm. All calculation parameters were grid spacing 0.3 cm, minimum segment width 1.0 cm, maximum 180 of control points per arc, fluence smoothing medium, statistical uncertainty 1.0% per calculation, increment of gantry 30o and calculate dose deposition to medium.
All patients were positioned supin with head toward the gantry. The VMAT-TBI tecnique consisted of three isocentres and three dual overlapping arcs. 75% of patients were pediatric, %25 of patients were adult and all patients were male in our study. We have treated adult patients with three dual overlapping arcs to the bottom of pelvic bone then we were positioned with feet toward the treatment gantry and we used 2 more overlapping arcs for whole body treatment. The prescribed dose was 90% of target volume receiving dose of 12 Gy. Mean dose to lungs and kidneys were restricted less than 10Gy and maximum dose to lens were restricted less than 6 Gy. The plans were verified using 2 Dimensional array IBA Matrixx® patient quality assurance (QA) system and CC13 ion chamber. The comparison between calculation and measurement were made by γ-index (3%-3 mm) analysis and absolute dose measurement at the isocentre.
When we compared five patient’s organ at risk (OAR)s doses for three VMAT techniques, we had less dose and better dose coverage to target with dual arc VMAT technique, it is shown Table 1. Segments, total MUs and duration of treatment comparison between VMAT tecniques are given Table 2. Also, Figure 2 shows dose distribution of one TBI treatment by dual VMAT technique on the coach.
An average total delivery time was determined 923 ± 34 seconds and an average monitor unit (MU)s was determined 2614 ± 231 MU for dual arc VMAT technique. When we evaluated organ at risk (OAR)s, mean dose to lungs was 9.73 ± 0.2 Gy, mean dose to kidneys was 8.89 ± 0.3 Gy, maximum dose to lens was 5.50 ± 0.3 Gy and maximum point dose was 14.59 ± 0.3 Gy, HI of PTV was 1.13 ± 0.02, mean dose to PTV was 12.60 ± 0.15 Gy and mean γ-index (3% - 3 mm) pass rate was %97.13 ± 1.9. These are shown Table 3.
The results show that dose coverage of target and OAR’s doses also depend significantly VMAT techniques. MLCs mostly move just one side of isocentre in first tour of VMAT then MLCs mostly move other side of isocentre in second tour of VMAT with dual arc VMAT technique, therefore this technique is decreasing MUs and delivery time of treatment, also a benefit could be demonstrated with regard to dose distribution and homogeneity and dose-reduction to organs at risk. We could use cone beam CT images and SGRT method for positioning and monitoring patients. The tecnique for TBI using dual arc VMAT on the treatment coach was found feasible. Additionally, we determined highly precise dose delivery by TBI patient’s quality assurace (QA) and point dose measurement. Total Marrow Irradiation (TMI) treatment is also possible with VMAT based treatment on the coach by linear accelerator. Based on the dose distributions we have decided to plan TBI in our clinic with dual arc VMAT technique on the treatment coach.

![]()

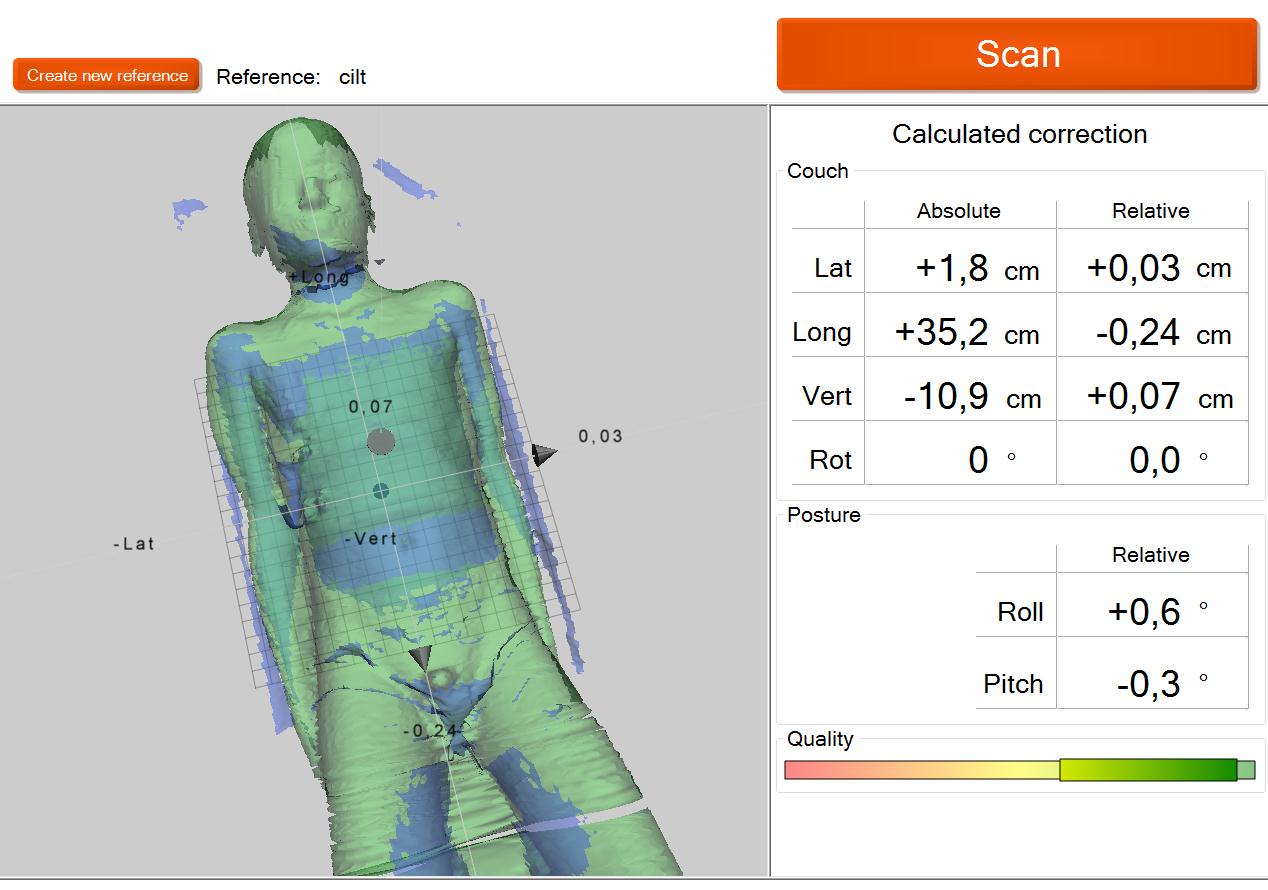 |
| Figure 1: One TBI patient's positioning and monitoring by Sentinel laser based SGRT scan |
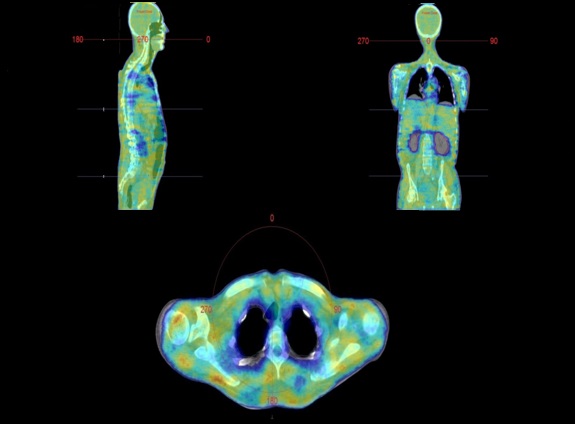 |
| Figure 2: Dose distribution of TBI treatment's sagital, coronal and axial plane by dual arc VMAT tecnique |
Single arc VMAT |
Two fields arc VMAT |
|||||||
|---|---|---|---|---|---|---|---|---|
Patient |
Lung R. |
Lung L. |
Kidney R. |
Kidney L. |
Lung R. |
Lung L. |
Kidney L. |
Kidney L. |
1 |
9.6% |
6.0% |
8.6% |
9.7% |
11.0% |
8.6% |
12.0% |
9.6% |
2 |
11.0% |
12.0% |
7.0% |
13.0% |
16.0% |
10.0% |
10.0% |
17.0% |
3 |
1.8% |
1.6% |
3.5% |
-1.0% |
4.7% |
4.5% |
4.0% |
4.0% |
4 |
4.2% |
4.0% |
6.7% |
7.6% |
-2.2% |
0.0% |
5.0% |
4.8% |
5 |
3.8% |
5.0% |
8.4% |
5.0% |
2.5% |
2.9% |
0.1% |
0.2% |
Mean±SD |
6.08±4.0% |
5.72±3.9% |
6.84±2.0% |
6.86±5.3% |
6.40±7.1% |
5.20±4.1% |
6.22±4.8% |
7.12±6.4% |
| Table 1: Mean doses of lungs and kidneys difference between dual arc VMAT and other tecniques | ||||||||
Dual arc VMAT |
Single arc VMAT |
Two fields arc VMAT |
|||||||
|---|---|---|---|---|---|---|---|---|---|
Patient |
Segments |
Total MUs |
Duration (seconds) |
Segments |
Total MUs |
Duration (seconds) |
Segments |
Total MUs |
Duration (seconds.) |
1 |
651 |
1903.33 |
847.56 |
452 |
2202.01 |
695.27 |
802 |
2992.15 |
1305.90 |
2 |
641 |
2286.86 |
723.55 |
422 |
2788.57 |
661.05 |
785 |
3299.35 |
1233.83 |
3 |
670 |
2042.11 |
800.69 |
473 |
2900.35 |
732.04 |
879 |
3653.44 |
1432.15 |
4 |
753 |
2573.09 |
908.33 |
456 |
2962.72 |
733.65 |
851 |
3298.61 |
1514.01 |
5 |
723 |
2207.01 |
895.84 |
473 |
2562.15 |
732.57 |
839 |
3397.92 |
1476.58 |
Mean±SD |
687.60±48 |
2202.48±255 |
835.19±76 |
455.20±21 |
2683.16±309 |
710.90±32 |
831.20±38 |
3328.29±237 |
1392.49±118 |
| Table 2: Number of segments, total MU’s and duration of treatment’s comparison between VMAT tecniques | |||||||||
Patient |
Lung R. (Gy) |
Lung L. (Gy) |
Kidney R. (Gy) |
Kidney L. (Gy) |
Lens R. (Gy) |
Lens L. (Gy) |
Max. Dose (Gy) |
Mean Dose of PTV (Gy) |
HI |
γ-index |
Total MUs |
Beam On (seconds) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
1 |
9.9 |
9.4 |
8.7 |
8.6 |
5.3 |
5.1 |
14.3 |
12.6 |
1.11 |
%96.2 |
2665.8 |
953.9 |
2 |
9.4 |
9.6 |
8.6 |
8.8 |
5.3 |
5.3 |
14.3 |
12.5 |
1.12 |
%94.3 |
2248.3 |
901.4 |
3 |
10.0 |
9.9 |
8.9 |
9.0 |
6.0 |
5.7 |
14.9 |
12.5 |
1.16 |
%99.2 |
2564.2 |
874.3 |
4 |
9.9 |
9.8 |
9.0 |
9.3 |
5.8 |
6.0 |
14.8 |
12.7 |
1.14 |
%97.6 |
2838.6 |
950.4 |
5 |
9.8 |
9.7 |
9.3 |
8.7 |
5.8 |
5.6 |
14.6 |
12.6 |
1.14 |
%98.2 |
2756.8 |
937.1 |
6 |
9.7 |
9.8 |
8.8 |
9.0 |
5.2 |
5.2 |
14.5 |
12.4 |
1.14 |
%98.1 |
2804.6 |
921.6 |
7 |
9.5 |
9.6 |
8.9 |
8.6 |
5.4 |
5.3 |
14.4 |
12.6 |
1.12 |
%94.7 |
2706.6 |
883.4 |
8 |
9.8 |
9.7 |
8.8 |
9.2 |
5.3 |
5.6 |
14.9 |
12.9 |
1.13 |
%98.7 |
2604.6 |
961.9 |
Mean±SD |
9.75±0.2 |
9.69±0.2 |
8.88±0.2 |
8.90±0.3 |
5.51±0.3 |
5.48±0.3 |
14.59±0.3 |
12.60±0.15 |
1.13±0.02 |
%97.13±1.9 |
2648.69±231 |
923±34 |
| Table 3: Dosimetric features of TBI by dual arc VMAT tecnique | ||||||||||||




































