Open Access
Research Article
Max Screen
ISSN: 2454-499X
Copyright: © 2018 Nabeel Nazeer. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Candida, a commensal of the oral and the vaginal cavity, sometimes turns invasive, in immunosuppressed individuals. The resultant lesion, known as invasive or aggressive candidiasis, can be extremely refractory to treatment.
This is a case report of an ulcero proliferative lesion in the hard palate that mimicked an intra-oral neoplasm. The clinical picture was confused by the fact that the patient was a chain smoker, and also because the initial MRI images were strongly suggestive of an invasive malignancy. When clinical and radiological signs exactly mimic a malignancy, the picture is confusing.
This is the case report of a 41year old with HIV who was presented with a tumour like ulceroproliferative lesion of the soft palate, with erosion and destruction of the maxilla, and with progression to the base of the skull, treated successfully with long term anti-fungal cocktail.
Keywords: HIV
Candida species are human fungal pathogens that cause mucosal and deep tissue infections. There is evidence to suggest that the majority of infections produced by this pathogen are associated with biofilm growth [1].Immuno compromised patients are prone to opportunistic infections. Lower CD4 count between 200-250 cells/mm3, age and gender are considered as predisposing factors for the increasing incidence rate [2]. The fungal group of infections are caused by Candida albicans (Horn et al., 2009) [1].Although oropharyngeal candidiasis is a common issue, ranking as a first line sign of HIV to AIDS conversion, only rarely is it invasive, mimicking a tumour in many ways. Invasive candidiasis has an increasing incidence and a crude mortality exceeding 50% [3].
This is a case report of an ulcero proliferative lesion in the hard palate that mimicked an intra-oral neoplasm. The clinical picture was confused by the fact that the patient was a chain smoker, and also because the initial MRI images were strongly suggestive of an invasive malignancy. Fortunately, after multiple biopsies, the hyphae of the candida were identified, and appropriate anti-fungal therapy instituted after which there was a marked diminision in size in the intra oral portion. This case is being presented because of its rarity, and in order to highlight the multiple aspects of aggressive candidiasis in the immuno suppressed.
A 41 year old, diagnosed with HIV three years prior to presentation, and on first line Highly Active Antiretroviral Therapy (HAART), presented with a non-healing ulcer of the soft palate. In the last three months, he had lost significant weight, and had a fall of CD4 count by 15%.He also had an increase in viral count, the latter two attributable to noncompliance with therapy for four months.
The ulceroproliferated area on the soft palate was 4 cms across, extending up to the uvula. The edge of the ulcer was everted, and unhealthy slough was seen in the base of the ulcer. The entire lesion was indurated, and bled to examination.
There was a diffuse fullness, pain and tenderness over the left maxilla, and the patient also complained of epistaxis. X-rays showed diffuse thickening of the wall of the maxillary sinus, and suggested involvement of the floor of the antrum. MRI of the skull and sinuses showed infiltration of the posterio inferior part of the left maxilla by a mass lesion. The posterior aspect extended to the base of the skull. Biopsies of the lesion were taken in four quadrants.
There was no histopathological evidence of malignancy, but dense inflammatory infiltrate with macrophages and leukocytes, was found in all four quadrants. Fungal stains revealed no hyphae (Figure 1).
As malignancy was ruled out, a provisional diagnosis of invasive candidiasis was made, and the patient was commenced on Itraconazole, 150 mg/day. The HAART was recommended, ensuring patient compliance this time.
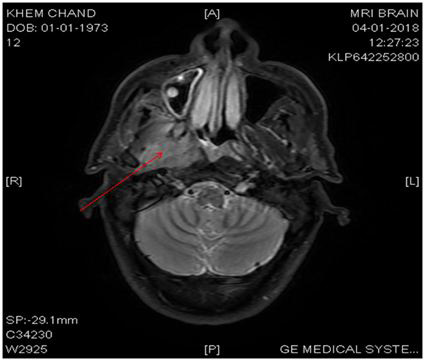
There was a partial improvement of the clinical picture, but not total regression. MRI was repeated 4 months after the administration of Itraconazole, and this showed extension of base of skull disease, but reduction of maxillary disease (Figure 2).
An ID consult was sought, and voriconazole was started. In the meantime, he developed palatial anesthesia on the left side, and a suspicion of malignant infiltration of the pterygo palatine fossa was brought up. Accordingly, he underwent multiple biopsies again, which showed the same histopathology as the first time, with no evidence of malignancy or obvious fungal hyphae.
High dose oral Itraconazole (250 mg) and ten day bursts of voriconazole were given for the next three months, and the palatal lesion regressed significantly. A third set of biopsies showed nil malignancy but this time fungal hyphae were obtained from scrapings of the maxillary wall. A fortnight’s course of Caspofungin was given, and the patient was then continued on oral Itraconazole.
At last review, nine months after initial presentation, he still has a residual lesion in the maxilla, but the palatal part has almost completely regressed. His HIV status has stabilized, with a viral count that is negligible and a CD4 count of 690cells/mm3 (Figure 3).
Opportunistic infections enter the body due to compromised host defense or through an invasive gateway. Candida infection is more often encountered fungal infection [4]. One third of the HIV positive patients suffer from oral candidiasis [5].
Candida infection develops due to the colonization of the mucocutaneous surfaces. Along with the increased colonization rate HIV is associated with the development of overt disease. During the course of HIV infection, the rate of Candida infection is inversely related to the CD4 counts of the patient which in turn determines the Anti-retroviral treatment [6]. Alterations in the number and differentiation of lymphocytes and dendritic cells play a role in the pathogenesis and evolution of the disease [7].
Candidiasis in HIV disease is no exception, being almost the norm. But invasive/aggressive candidiasis is a different entity, infiltrating surrounding structures, and behaving exactly like a locally invasive malignancy.
This case is educative from many aspects:
The discontinuation of the HAART by the patient probably set off a chain of events, from lowered CD 4 and increased viral counts, triggering off an invasive response by the Candida.
The MRI films were ambivalent, and the invasion of the maxilla and the skull base were highly suggestive of malignancy, warranting multiple biopsies, that were negative for neoplasm. The fact that only the third set of biopsies showed fungal hyphae, points to the innate difficulties of fungus diagnosis. Scrapings from the expanding side of the lesion, will demonstrate fungi, and this was the case here.
This case study is significant for the following reasons – 1. Fungus, especially invasive candiasis can mimic tumour in the immunosuppressed individual. In an era of increasing HIV disease this is an important message. 2. If repeated biopsies of a tumour like lesion turn out to be negative one has to consider rarer conditions like an invasive fungus .3. Avoidance of aggressive procedures in the immunosuppressed groups of patients without a definite tissue diagnosis is a caveat.
Invasive/aggressive Candidiasis, in immune compromised patients, can mimic malignancy. This case report of an Indian patient with aggressive Candidiasis of the palate, that reached the base of the skull, is reported for its unique diagnostic and therapeutic difficulties.

![]()

 |
| Figure 1: Before |
 |
| Figure 2: After |
 |
| Figure 3: |




































